Pharmaceutical Sciences. 31(4):480-490.
doi: 10.34172/PS.025.42849
Research Article
PPARγ Role on Ameliorating the Effects of Losartan in LPS-Induced Lung and Systemic Injuries in Mice
Mohammad Hossein Boskabady Funding acquisition, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, 1, 2, * 
Vajiheh Rouki Investigation, Methodology, Project administration, 2
Saeideh Saadat Data curation, Investigation, Methodology, Project administration, Validation, 3
Arghavan Memarzia Data curation, Investigation, Methodology, Project administration, Software, Validation, 1, 2
Hossein Salmani Data curation, Project administration, 2
Nema Mohammadian Roshan Data curation, Project administration, 4
Zahra Gholamnezhad Data curation, Project administration, 1, 2
Mahmoud Hosseini Data curation, Project administration, 1, 2
Author information:
1Applied Biomedical Research Center, Basic Sciences Research Institute, Mashhad University of Medical Sciences, Mashhad, Iran
2Department of Physiology, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran
3Department of Physiology, School of Medicine, Zahedan University of Medical Sciences, Zahedan, Iran
4Department of Pathology, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran
Abstract
Background:
The effects of losartan (Los) and GW9662 on lipopolysaccharides (LPS)-induced acute lung injury (ALI) and systemic inflammation were examined.
Methods:
Mice were administered saline or LPS (0.250 mg/kg) for seven days and were treated with Los (1 mg/kg), GW9662 (1 mg/kg), or their combination for ten days (n=7 per group). Total and differential white blood cells (WBC) in the blood and the bronchoalveolar lavage fluid (BALF), oxidant and anti-oxidant markers including malondialdehyde (MDA), total thiol, superoxide dismutase (SOD), and catalase (CAT) levels were measured in serum, the levels of interleukin-4 (IL-4), interferon gamma (IFN-γ), and transforming growth factor beta (TGF-β1) in the BALF, and lung histopathological changes were assessed.
Results:
In the LPS group, SOD, CAT, and thiol in serum, and TGF-β1 and IFN-γ levels and INF-γ/IL-4 ratio in the BALF were decreased, but WBC count in the blood and BALF, and serum MDA, BALF IL-4 level and lung pathological changes were significantly increased. Most variables were improved in the LPS group treated with Los or its combination with GW9662. Treatment with GW9662 alone did not change any variable.
Conclusion:
Although the preventive effect of Los may not be entirely mediated through the PPAR-γ receptor, the results indicate that the Los effect is partially reversed with GW9662 treatment, suggesting at least a partial involvement of the PPAR-γ pathway.
Keywords: Losartan, Angiotensin II receptor antagonist, PPAR-γ-receptor antagonist, Lipopolysaccharides, Lung injury, Oxidative stress, Inflammation
Copyright and License Information
© 2025 The Author(s).
This is an open access article and applies the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
National Institute financially supported this study for Medical Research Development (NIMAD. Project 943735).
Introduction
Several factors such as environmental pollutants, and bacterial and viral infections may induce lung inflammation leading to chronic obstructive pulmonary disease (COPD).1,2 Inflammatory markers including cytokines3-5 and growth factors can induce pathological changes in lung tissue by promoting tissue fibrosis6 which causes acute lung injury (ALI).7 It was shown that tobacco products8 and pollutants9 are potential sources of lipopolysaccharide (LPS).
LPS is the main biological component of the cell membrane of Gram- negative bacteria and it can induce ALI by increasing pro-inflammatory mediators and oxidative stress markers.10 The levels of interleukin one beta (IL-1β), tumor necrosis factor-alpha (TNF-α), IL-6, and autophagy were shown to increase in LPS-induced ALI in mice and A549 epithelial cells of human alveoli.11 Inducing ALI by LPS via stimulating pro-inflammatory cytokine production and activation of Toll-like receptor (TLR4) and TLR2 dependent signaling pathways was indicated.7 In the LPS-induced ALI mice, miR-126-5p plays a crucial role in down-regulating vascular endothelial growth factor-A (VEGFA), which is typically overexpressed during ALI and contributes to increased vascular permeability and inflammation; thus, the downregulation of miR-126-5p leads to VEGFA overexpression that exacerbates lung injury, while restoration of miR-126-5p alleviates ALI by maintaining endothelial integrity and reducing inflammation.12 Moreover after LPS administration, fibrotic factors including TGF-β1, collagen type I and III, and α-smooth muscle-actin (α-SMA) levels were reported to increase.13
Losartan (Los), as an angiotensin II receptor antagonist, is a medication mainly used to treat cardiac failure and hypertension which are common comorbidities in COPD patients. This drug showed therapeutic effect on COPD by decreasing pneumonia and exacerbation factors which reduced the mortality rate in COPD.13-18 Treatment with Los also decreased inflammation, oxidative stress, and nuclear factor kappa B (NF-κB) protein expression in COPD rats with ALI induced by tobacco smoke.19
In addition, the ameliorative effect of PPAR-γ agonist on LPS-induced neuro-inflammation was demonstrated. It was indicated that treatment with PPAR-γ agonist decreases the expression of inflammatory mediators and the expression of their related signaling proteins such as IκB and NF-κβ.20
Therefore, the present study aimed to examine the effects of Los alone or in combination with a PPAR-γ-receptor antagonist on ALI and inflammation induced by LPS. This aim was achieved by assessing the therapeutic effects of an angiotensin II receptor antagonist, Los alone, and in the presence of a PPAR-γ receptor antagonist, GW9662 on LPS-induced ALI.
Materials and Methods
Animals
In the animal house of Mashhad University of Medical Sciences, Mashhad, Iran, BALB/c mice (male, 30-35 g) were kept in cages (temperature of 22 ± 2 °C, humidity of 54 ± 2% and light/dark cycle 12 h). Animal experimental protocols (code 951071) were approved by the ethics committee of Mashhad University of Medical Sciences. National Laws regarding the use and care of laboratory animals complying with the ARRIVE guidelines by either the U.K. Animals (Scientific Procedures) Act, 1986 and associated guidelines, the EU Directive 2010/63/EU for animal experiments, or the National Research Council’s Guide for the Care and Use of Laboratory Animals were followed.
Experimental Groups
Seven groups of mice in two main categories were included in the study (n = 7 in each group) as follows:
simple
-
A) Saline-administered groups including:
simple
-
1. Non-treated or control (Ctrl) group
-
2. Los (1 mg/kg/day, 10 days)-treated (Los) group
-
3. GW9662, a PPAR-γ receptor antagonist (1 mg/kg/day)-treated (GW) group
-
B) LPS-administered (0.25 mg. kg/day, 7 days) groups including:
simple
-
4. Non-treated (LPS) group
-
5. Group treated with Los (LPS-Los)
-
6. Group treated with GW9662 (LPS-GW)
-
7. Group treated with a combination of GW9662 and Los (LPS-GW-Los)
Los (1 mg/kg) and GW9662 (1 mg/kg) were administered for ten days intraperitoneally (i.p.) and saline or LPS (250 μg/kg, i.p.) were injected during the last seven days (18) (Figure 1).
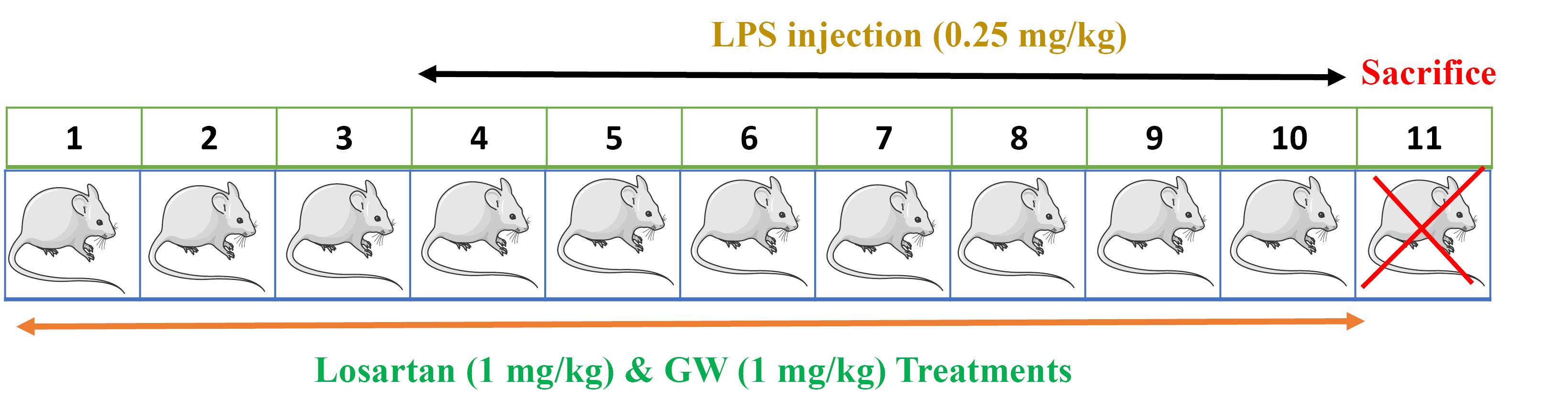
Figure 1.
Time table of the study and protocol of lipopolysaccharide (LPS)-induced lung injury and treatment (The form of the rat used on the site https://smart.servier.com/ and final drawing of the software Power Point).
.
Time table of the study and protocol of lipopolysaccharide (LPS)-induced lung injury and treatment (The form of the rat used on the site https://smart.servier.com/ and final drawing of the software Power Point).
On day 11 (the end of the experiment), ketamine (50 mg/kg, i.p.)21 and xylazine (5 mg/kg, i.p.)21 were injected and animals were sacrificed without pain and stress. The lungs were removed, the left lung was clamped and the right lung was washed five times through a tracheal cannula, each time with 1 mL saline (5 ml, total) for preparing BALF. To measure the cytokine levels (IL-4, IFN-γ, and TGF-β) as well as oxidative stress markers, the BALF was centrifuged for 10 min at 2500 rpm, at 4 °C and the supernatant was stored at -70 °C. After animals were sacrificed, a blood sample (2.5 mL) was prepared from the heart, its serum was isolated, and total and differential WBC were counted according to a previous method.22 To measure oxidative stress markers, the BALF samples were prepared and stored at -70 °C.
Counting White Blood Cells (WBC)
Total WBC was counted in a hemocytometer (Burker chamber) in the blood and the BALF. The smear of blood was stained with Wright-Giemsa and differential WBC was counted based on a previous method.21
Assessment of Oxidative Stress
Oxidant and anti-oxidant markers including MDA, total thiol, SOD, and CAT levels were measured in serum samples stored at -70 based on a previously reported method21,23 and described below.
MDA was measured using, 2 mL reagent of thiobarbituric acid (TBA)/trichloroacetic acid (TCA)/HCl added to 1 ml serum and heated in a water bath for 40 min and cooled and centrifuged at 1000 × g for 10 min. At 535 nm, the absorbance was measured and MDA concentration (C) in nM was calculated using C = Absorbance/ (1.56 × 105).
Measurement of the activity of SOD was done by the generation of superoxide by pyrogallol auto-oxidation and the inhibition of superoxide-dependent reduction of the tetrazolium dye, MTT (3-(4, 5-dimethylthiazol-2-yl, 2, 5-diphenyltetrazolium bromide) to its formazan by SOD. At 570 nm, SOD activity was measured and expressed as unit (U)/mL.
Measurement of the activity of CAT was done by determination of the rate constant, k, (dimension: s-1, k) of hydrogen peroxide decomposition by the reduction in absorbance at 240 nm per minute and expressed as unit (U)/mL.
Measurement of total thiol concentration was done by adding 1 ml trisethylene diamine tetraacetic acid (EDTA) buffer to 50 μL serum in 1 ml cuvettes and read at 412 nm against Tris-EDTA buffer alone (A1). Then, 20 μL DTNB reagents were added to the mixture and kept for 15 min and the sample absorbance was read again (A2). The absorbance of the DTNB reagent was read as a blank (B) and the following equation was used to calculate total thiol concentration (mM):
Total thiol concentration (mM) = (A2–A1–B) × 1.07/0.05 × 13.6.
Measurement of Cytokine Levels
The levels of IL-4 (Catalogue Number: SRP3211), IFN-γ (Catalogue Number: SRP3058), and TGF-β1(Catalogue Number: SRP0300) in the BALF were evaluated using specific ELISA kits (eBioscience Co, San Diego, CA, USA) based on the manufacturer’s instructions and a previous method.
Evaluation of Lung Histopathological Changes
Lung histopathological change scores including interstitial inflammation, fibrosis, lymphoid infiltration, and emphysema were evaluated in the left lung based on a previous method.21,24 The specimens of the left lung were fixed in 10% formalin (37%, Merck, Germany), embedded in paraffin and cut into 4 μm sliced then they were stained with hematoxylin-eosin (H&E) solution and pathological evaluations were done under a light microscope. Lung pathologic changes were scored as: no pathologic changes = 0, patchy changes = 1, local changes = 2, scattered changes = 3 and severe changes (in the most parts of the lung) = 4. Lung pathological evaluation was performed in the control, LPS, LPS-Los, LPS-GW, and LPS-GW-Los groups because there were minor changes in the other measured variables in the Saline-Los, and Saline-GW groups.
Statistical Analysis
Mean ± SEM of the data is presented and compared among groups using ANOVA (one-way analysis of variance) and Tukey post hoc test. The level of P < 0.05 was regarded as statistical significance.
Results
Systemic Results
Blood WBC Results
The numbers of WBC (total and differential) were significantly increased in the LPS group (P < 0.001 for all cases) but the Saline-Los and Saline-GW groups did not show significant changes in total and differential WBC compared to the Ctrl group (Figure 2).
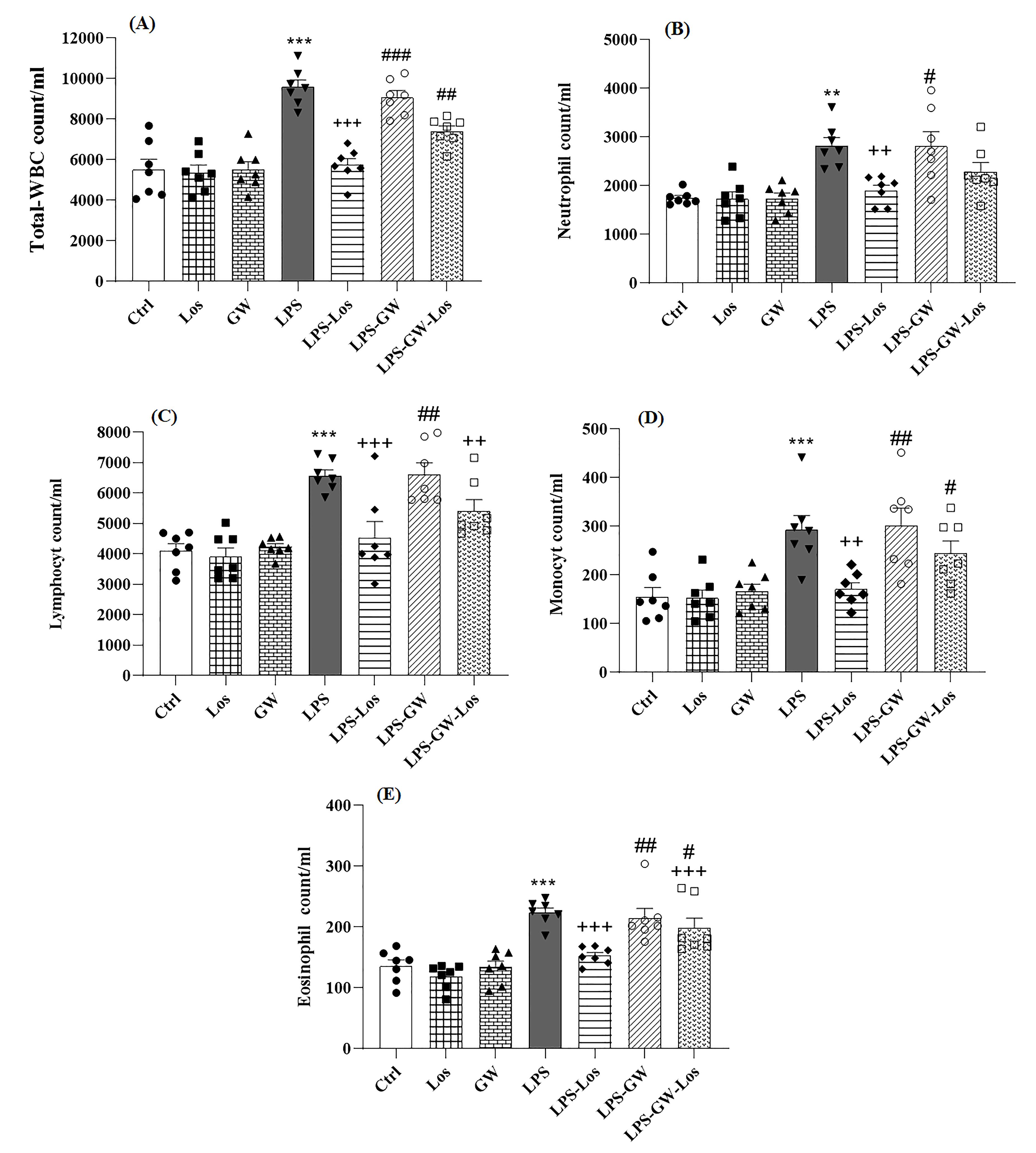
Figure 2.
Total WBC (A) neutrophil (B) Lymphocyte (C) Monocyte (D), and Eosinophil (E) counts in the blood examined by cell counting of the control (Ctrl(, saline + losartan (1 mg/kg)-treated (Los), saline + GW9662 (1 mg/kg)-treated (GW), lipopolysaccharid-administered (LPS), LPS + Los (1 mg/kg)-treated (LPS-Los), LPS + GW9662 (1 mg/kg)-treated (LPS-GW), and LPS + Los + GW9662 combination-treated (LPS-GW-Los) groups. Data are shown as mean ± SEM (n = 7 per group). **; P < 0.01 and ***; P < 0.001 compared to the control group, + + ; P < 0.01 and + + + ; P < 0.001 compared to the LPS group, #; P < 0.05 and ##; P < 0.01, ###; P < 0.001 compared to the LPS-Los group. Statistical analysis were performend using one-way analysis of variance (ANOVA) followed by Tukey’s multiple comparison test.
.
Total WBC (A) neutrophil (B) Lymphocyte (C) Monocyte (D), and Eosinophil (E) counts in the blood examined by cell counting of the control (Ctrl(, saline + losartan (1 mg/kg)-treated (Los), saline + GW9662 (1 mg/kg)-treated (GW), lipopolysaccharid-administered (LPS), LPS + Los (1 mg/kg)-treated (LPS-Los), LPS + GW9662 (1 mg/kg)-treated (LPS-GW), and LPS + Los + GW9662 combination-treated (LPS-GW-Los) groups. Data are shown as mean ± SEM (n = 7 per group). **; P < 0.01 and ***; P < 0.001 compared to the control group, + + ; P < 0.01 and + + + ; P < 0.001 compared to the LPS group, #; P < 0.05 and ##; P < 0.01, ###; P < 0.001 compared to the LPS-Los group. Statistical analysis were performend using one-way analysis of variance (ANOVA) followed by Tukey’s multiple comparison test.
The numbers of WBC (total and differential) in the LPS-Los group were significantly decreased in comparison with the LPS group (P < 0.01 for neutrophils and monocytes and P < 0.001 for other cases) (Figure 2).
In the LPS-GW-Los group, lymphocytes (P < 0.01) and eosinophils were significantly decreased compared to the LPS group (P < 0.001) (Figure 2). The effects of GW-Los combination treatment on total and differential WBC were significantly lower than that of Los treatment except for monocytes count (P < 0.05 for neutrophils and P < 0.01 for other cases) (Figure 2).
However, the numbers of WBC (total and differential) in the LPS-GW group were not changed compared to the LPS group (Figure 2). In addition, in the LPS-GW group, total and differential WBC counts were significantly higher than the LPS-Los group (P < 0.05 to P < 0.001) (Figure 2).
Increased total and differential WBC in the blood in the LPS group indicated LPS-induced systemic inflammation. The reduction in systemic inflammation (total and differential WBC) observed in the LPS-treated group receiving both Los and GW highlights the therapeutic effect of Los, which is further enhanced by the additive effect of GW.
Serum Oxidant and Anti-Oxidant Markers
Significantly decreased serum CAT and SOD activities and thiol levels but increased MDA levels, were observed in the LPS group compared to the control group (P < 0.001 for all cases). However, there were no significant changes in oxidative stress markers in the Saline-Los and Saline-GW groups in comparison to the Ctrl group (Figure 3).
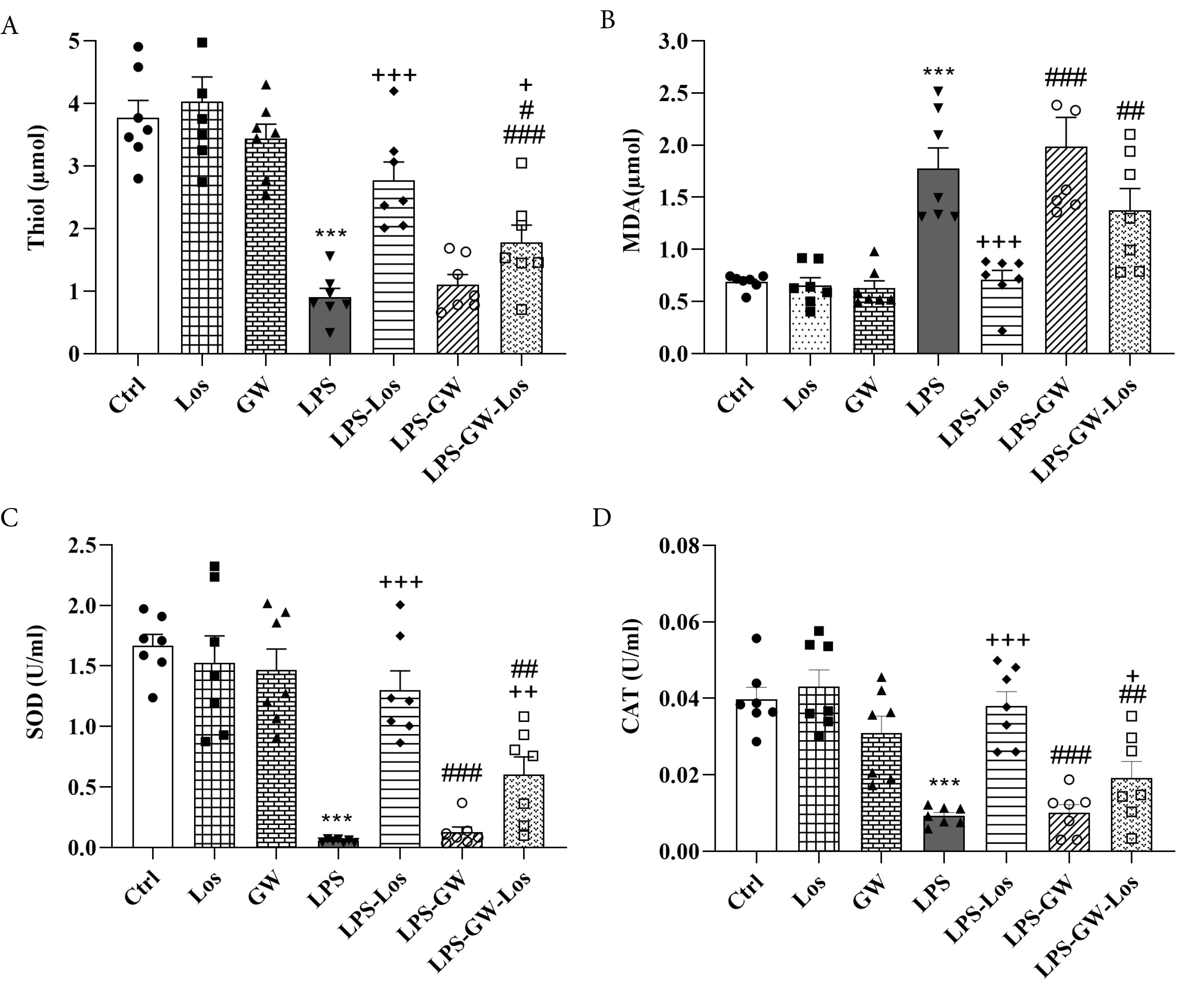
Figure 3.
The levels oftotal thiol (A) MDA (B) SOD (C) and CAT (D) in the serum examined by cell biochemical methods of the control (Ctrl), saline + losartan (1 mg/kg)-treated (Los), saline + GW9662 (1 mg/kg)-treated (GW), lipopolysaccharid-administered (LPS), LPS + Los (1 mg/kg)-treated (LPS-Los), LPS + GW9662 (1 mg/kg)-treated (LPS-GW), and LPS + Los + GW9662 combination-treated (LPS-GW-Los) groups. Data are shown as mean ± SEM (n = 7 per group). ***; P < 0.001 compared to the control group, + ; P < 0.05 and + + ; P < 0.01, + + + ; P < 0.001 compared to the LPS group, #; P < 0.05 ##; P < 0.01 and ###; P < 0.001 compared to the Los group. Statistical analysis were performend using one-way analysis of variance (ANOVA) followed by Tukey’s multiple comparison test.
.
The levels oftotal thiol (A) MDA (B) SOD (C) and CAT (D) in the serum examined by cell biochemical methods of the control (Ctrl), saline + losartan (1 mg/kg)-treated (Los), saline + GW9662 (1 mg/kg)-treated (GW), lipopolysaccharid-administered (LPS), LPS + Los (1 mg/kg)-treated (LPS-Los), LPS + GW9662 (1 mg/kg)-treated (LPS-GW), and LPS + Los + GW9662 combination-treated (LPS-GW-Los) groups. Data are shown as mean ± SEM (n = 7 per group). ***; P < 0.001 compared to the control group, + ; P < 0.05 and + + ; P < 0.01, + + + ; P < 0.001 compared to the LPS group, #; P < 0.05 ##; P < 0.01 and ###; P < 0.001 compared to the Los group. Statistical analysis were performend using one-way analysis of variance (ANOVA) followed by Tukey’s multiple comparison test.
All serum oxidative stress marker levels in the LPS-Los and LPS-GW-Los groups were significantly improved in comparison with the LPS group except MDA in the LPS-GW-Los group (P < 0.05 to P < 0.001) (Figure 3). The improvement of all oxidative stress markers in the LPS-Los group was significantly greater than that of the LPS-GW, and the improvement of SOD and CAT activities was higher than that of the LPS-GW-Los group (P < 0.05 to P < 0.01) (Figure 3).
The LPS-GWs groups did not show any significant improvement in oxidative stress markers compared to the LPS group (Figure 3).
The alterations in serum oxidative stress markers in the LPS group confirmed LPS-induced systemic oxidative stress. Treatment with Los improved these markers, and the combination of Los and GW resulted in even greater improvements, demonstrating both the protective effect of Los and the additive benefit of GW against LPS-induced oxidative stress.
Lung-Specific Results
WBC Results
In the LPS group, the numbers of WBC (total and differential) were increased in the BALF in comparison with the Ctrl group (P < 0.001 for all cases) but in the Saline-Los and Saline-GW groups, the numbers of WBC (total and differential) were not significantly changed in comparison with the Ctrl group (Figure 4).
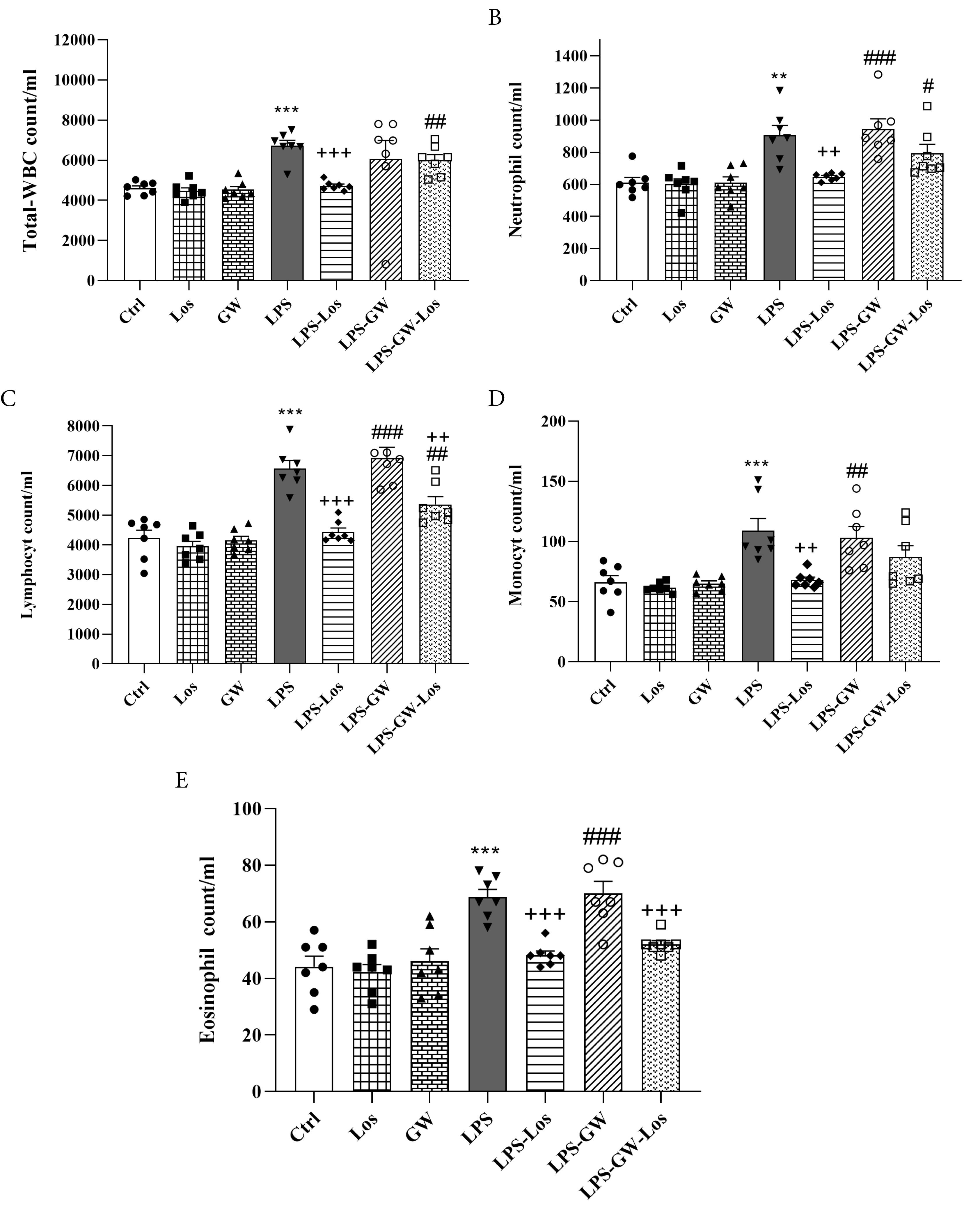
Figure 4.
Total WBC (A) Neutrophil (B) Lymphocyte (C), Monocyte (D), and Eosinophil (E) counts in the BALF examined by cell counting of the control (Ctrl), saline + losartan (1 mg/kg)-treated (Los), saline + GW9662 (1 mg/kg)-treated (GW), lipopolysaccharid-administered (LPS), LPS + Los (1 mg/kg)-treated (LPS-Los), LPS + GW9662 (1 mg/kg)-treated (LPS-GW), and LPS + Los + GW9662 combination-treated (LPS-GW-Los) groups. Data are shown as mean ± SEM (n = 7 per group). **; P < 0.01 and ***; P < 0.001 compared to the control group, + + ; P < 0.01 and + + + ; P < 0.001 compared to the LPS group, #; P < 0.05, ##; P < 0.01 and ###; P < 0.001 compared to the LPS-Los group. Statistical analysis were performend using one-way analysis of variance (ANOVA) followed by Tukey’s multiple comparison test.
.
Total WBC (A) Neutrophil (B) Lymphocyte (C), Monocyte (D), and Eosinophil (E) counts in the BALF examined by cell counting of the control (Ctrl), saline + losartan (1 mg/kg)-treated (Los), saline + GW9662 (1 mg/kg)-treated (GW), lipopolysaccharid-administered (LPS), LPS + Los (1 mg/kg)-treated (LPS-Los), LPS + GW9662 (1 mg/kg)-treated (LPS-GW), and LPS + Los + GW9662 combination-treated (LPS-GW-Los) groups. Data are shown as mean ± SEM (n = 7 per group). **; P < 0.01 and ***; P < 0.001 compared to the control group, + + ; P < 0.01 and + + + ; P < 0.001 compared to the LPS group, #; P < 0.05, ##; P < 0.01 and ###; P < 0.001 compared to the LPS-Los group. Statistical analysis were performend using one-way analysis of variance (ANOVA) followed by Tukey’s multiple comparison test.
Treatment with Los significantly reduced the numbers of WBC (total and differential) and treatment with the combination of GW-Los reduced monocyte and eosinophil counts (P < 0.01 to P < 0.001) in comparison with the LPS group (Figure 4). However, the effects of Los treatment on total and all differential WBC were significantly greater than GW-Los and combination treatment groups (P < 0.05 to P < 0.01) (Figure 4).
The numbers of WBC (total and differential) in the LPS-GW group were not changed in comparison with the LPS group (Figure 4). In the LPS-GW group, differential WBC counts were significantly greater than the LPS-Los group (P < 0.01 for monocyte and P < 0.001 for other cases) (Figure 4).
In the LPS group, total and differential WBC in the BALF were increased, indicating LPS-induced lung inflammation in terms of increased inflammatory cells. However, in the LPS group treated with Los, total and differential WBC were reduced which demonstrated the effect of Los on LPS-induced increased inflammatory cells in the lung.
BALF Cytokine Levels
In the LPS group, the levels of IFN-γ and TGF-β and INF-γ/IL-4 ratio in the BALF were significantly increased but the IL-4 level was decreased in comparison with the Ctrl group (P < 0.001 for all cases). In addition, the cytokine levels in the Saline-Los and Saline-GW groups did not change in comparison with the Ctrl group (Figure 5).
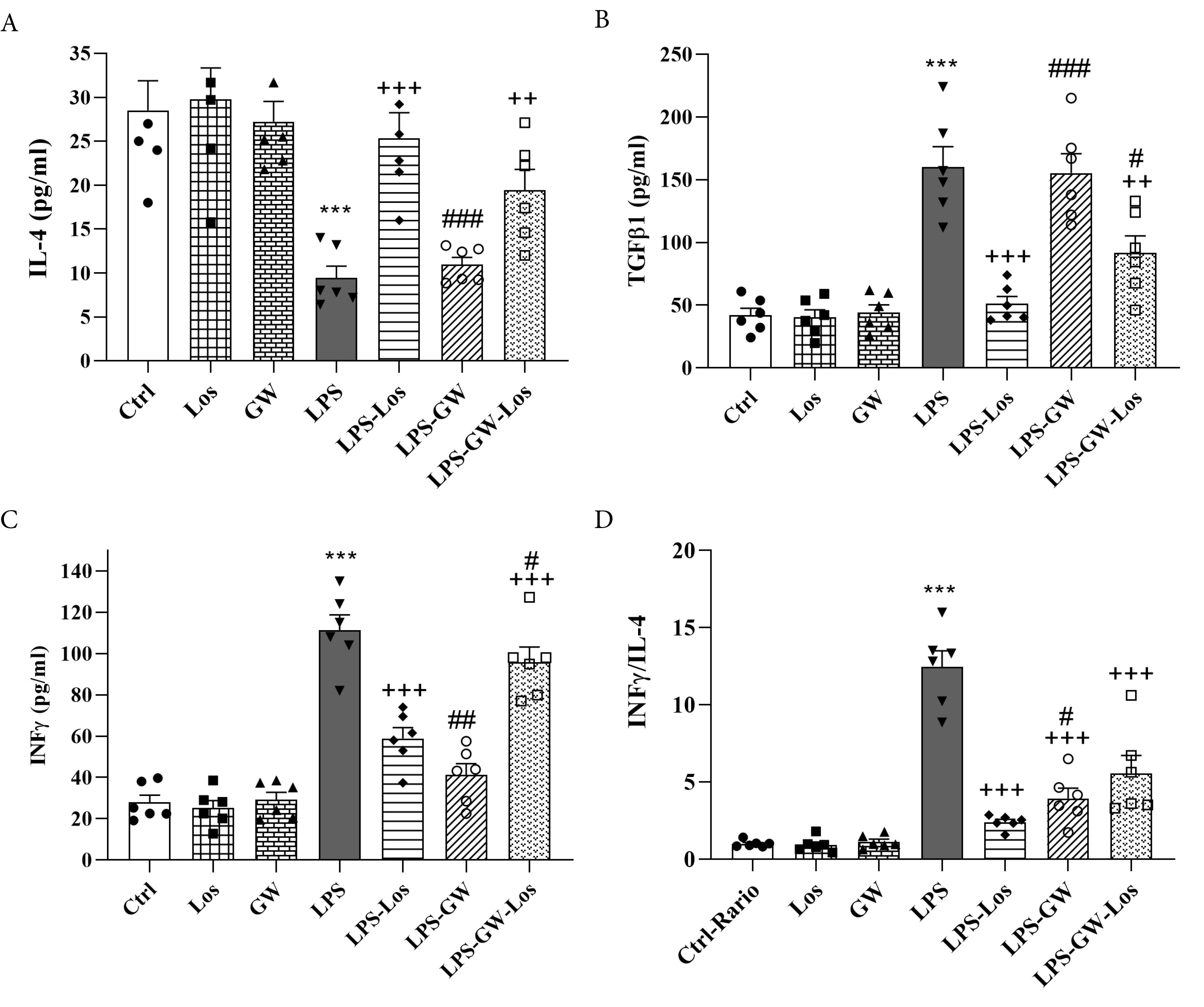
Figure 5.
IL-4 (A) TGF-β (B) and IFN-γ (C) INF-γ/IL-4 ratio (D) in the BALF examined by ELISA method of the control (Ctrl), saline + losartan (1 mg/kg)-treated (Los), saline + GW9662 (1 mg/kg)-treated (GW), lipopolysaccharid-administered (LPS), LPS + Los (1 mg/kg)-treated (LPS-Los), LPS + GW9662 (1 mg/kg)-treated (LPS-GW), and LPS + Los + GW9662 combination-treated (LPS-GW-Los) groups. Data are shown as mean ± SEM (n = 7 per group). ***; P < 0.001 compared to the control group, + + ; P < 0.01 and + + + ; P < 0.001 compared to the LPS group, #; P < 0.05, ##; P < 0.01, ###; P < 0.001 compared to the LPS-Los group. Statistical analysis were performend using one-way analysis of variance (ANOVA) followed by Tukey’s multiple comparison test.
.
IL-4 (A) TGF-β (B) and IFN-γ (C) INF-γ/IL-4 ratio (D) in the BALF examined by ELISA method of the control (Ctrl), saline + losartan (1 mg/kg)-treated (Los), saline + GW9662 (1 mg/kg)-treated (GW), lipopolysaccharid-administered (LPS), LPS + Los (1 mg/kg)-treated (LPS-Los), LPS + GW9662 (1 mg/kg)-treated (LPS-GW), and LPS + Los + GW9662 combination-treated (LPS-GW-Los) groups. Data are shown as mean ± SEM (n = 7 per group). ***; P < 0.001 compared to the control group, + + ; P < 0.01 and + + + ; P < 0.001 compared to the LPS group, #; P < 0.05, ##; P < 0.01, ###; P < 0.001 compared to the LPS-Los group. Statistical analysis were performend using one-way analysis of variance (ANOVA) followed by Tukey’s multiple comparison test.
Cytokines levels and INF-γ/IL-4 ratio were improved in the LPS-Los and LPS-GW-Los groups in comparison with the LPS group (P < 0.01 for TGF-β in the LPS-GW-Los group, and p < 0.001 for other cases), (Figure 5). The effect of GW-Los combination treatment on all measured cytokines and INF-γ/IL-4 ratio was significantly lower than Los alone (P < 0.05 to P < 0.001), (Figure 5).
There was no significant difference in cytokine levels in the LPS-GW group in comparison with the LPS groups (Figure 5).
Increased IFN-γ, TGF-β, and INF-γ/IL-4 ratio in the BALF but decreased IL-4 in the LPS group, are other important indicators of LPS-induced lung inflammation. The improvements in the cytokine levels and INF-γ/IL-4 ratio in the LPS group treated with Los have demonstrated the effect of Los on LPS-induced lung inflammation.
Lung Pathological Evaluation
Figure 6 illustrates photographs of lung histology in the Ctrl, LPS-Los, LPS-GW, and LPS-GW-Los groups. In the LPS group, interstitial inflammation, emphysema, lymphoid infiltration, and peri-bronchitis were significantly higher than in the Ctrl group (P < 0.001 for all cases) (Figure 6).
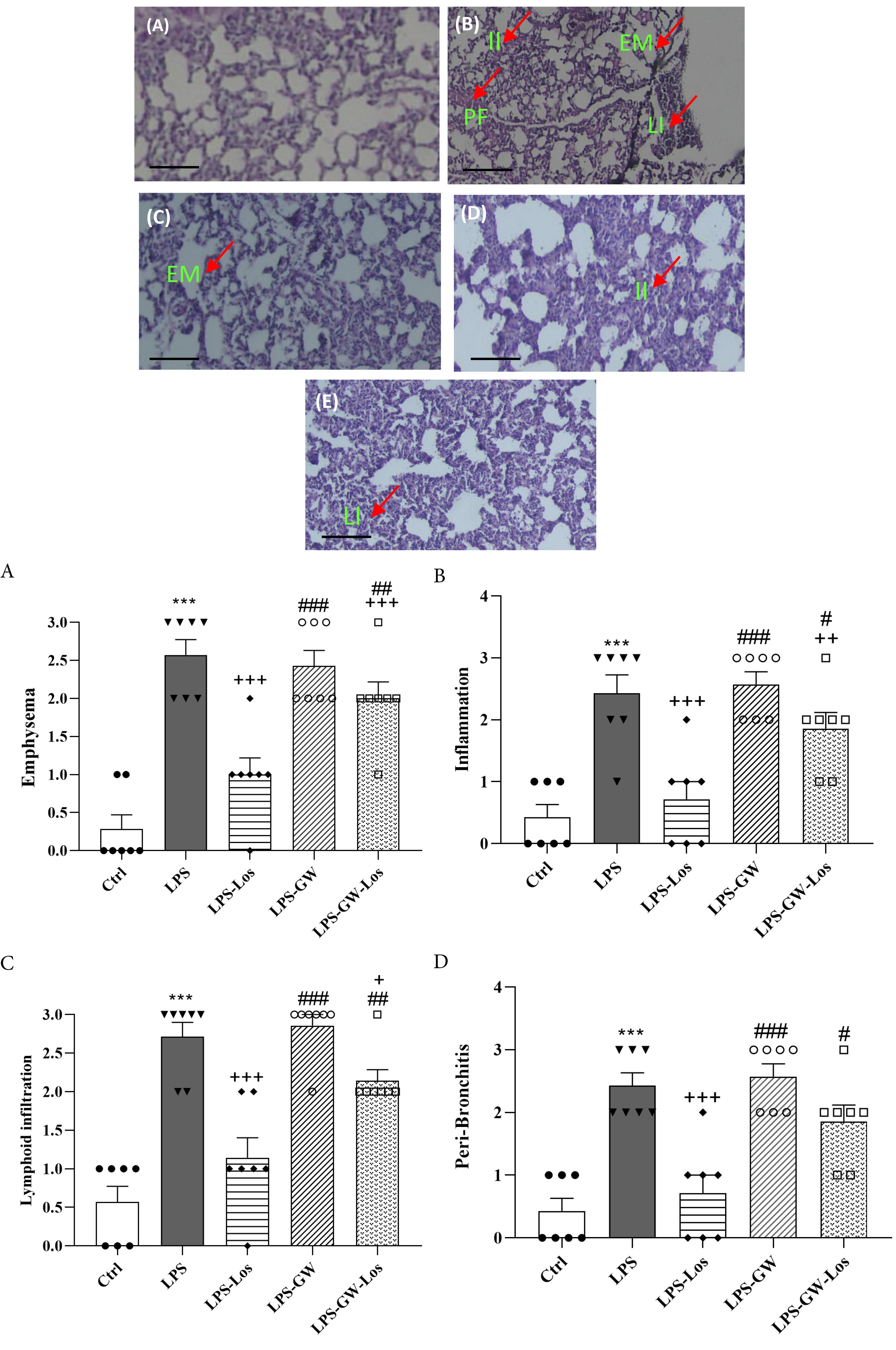
Figure 6.
Photographs of a lung specimen in the control (A), LPS (B), LPS-Los (C), LPS-GW (D), and LPS-GW-Los (E) groups indicating interstitial fibrosis (PE), interstital inflammation (II), lymphoid infiltration (LI) and emphysema (EM) (Magnification × 200, Scale bar = 10µm). Emphysema (A) and interstital inflammation (B), lymphoid infiltration (C), peri-bronchitis (D) of lung tissue examined by pathological methods (upper panel) in the control (Ctrl), saline + losartan (1 mg/kg)-treated (Los), saline + GW9662 (1 mg/kg)-treated (GW), lipopolysaccharid-administered (LPS), LPS + Los (1 mg/kg)-treated (LPS-Los), LPS + GW9662 (1 mg/kg)-treated (LPS-GW), and LPS + Los + GW9662 combination-treated (LPS-GW-Los) groups and their score (lower panel). Data are shown as mean ± SEM (n = 7 per group). ***; P < 0.001 compared to the control group, + ; P < 0.05, + + ; P < 0.01 and + + + ; P < 0.001 compared to the LPS group, #; P < 0.05, ##; P < 0.01, ###; P < 0.001 compared to the LPS-Los group. Statistical analysis were performend using one-way analysis of variance (ANOVA) followed by Tukey’s multiple comparison test
.
Photographs of a lung specimen in the control (A), LPS (B), LPS-Los (C), LPS-GW (D), and LPS-GW-Los (E) groups indicating interstitial fibrosis (PE), interstital inflammation (II), lymphoid infiltration (LI) and emphysema (EM) (Magnification × 200, Scale bar = 10µm). Emphysema (A) and interstital inflammation (B), lymphoid infiltration (C), peri-bronchitis (D) of lung tissue examined by pathological methods (upper panel) in the control (Ctrl), saline + losartan (1 mg/kg)-treated (Los), saline + GW9662 (1 mg/kg)-treated (GW), lipopolysaccharid-administered (LPS), LPS + Los (1 mg/kg)-treated (LPS-Los), LPS + GW9662 (1 mg/kg)-treated (LPS-GW), and LPS + Los + GW9662 combination-treated (LPS-GW-Los) groups and their score (lower panel). Data are shown as mean ± SEM (n = 7 per group). ***; P < 0.001 compared to the control group, + ; P < 0.05, + + ; P < 0.01 and + + + ; P < 0.001 compared to the LPS group, #; P < 0.05, ##; P < 0.01, ###; P < 0.001 compared to the LPS-Los group. Statistical analysis were performend using one-way analysis of variance (ANOVA) followed by Tukey’s multiple comparison test
All lung pathological changes were decreased in the LPS-Los group compared to the LPS group (P < 0.001 for all cases). The improvement of all pathological changes in the LPS-Los group was higher than in the LPS-GW-Los and LPS-GW groups (P < 0.05 to p < 0.001) (Figure 6).
The lung pathological changes in the LPS group showed LPS-induced ALI and their improvements in the LPS group treated with Los demonstrated the therapeutic effect of Los on LP-induced ALI.22
Correlation Between the BALF and Serum Total and Differential WBC Counts
There were significant correlations between the BALF and blood total and differential WBC counts (r = 0.82, 0.83, 0.76, 0.89, and 0.76 for total WBC, neutrophil, lymphocyte, eosinophil, and monocyte respectively, P < 0.001 for all cases) in the control LPS and treated groups. These correlations also suggested the parallel treatment effect of Los and GW on systemic and lung inflammation induced by LPS. These results indicate a connection between systemic and lung inflammation and demonstrate that systemic administration of LPS can induce both systemic and lung inflammations.
Discussion
In this study, LPS administration for 7 days increased the numbers of WBC (total and differential) in the blood and BALF, and serum level of MDA as well as BALF levels of IFN-γ, TGF-β and INF-γ/IL-4 ratio, but decreased BALF level of IL-4, total thiol content, and SOD and CAT activities in the serum. LPS exposure also induced lung pathological changes including intestinal inflammation, emphysema, lymphoid infiltration and peri-bronchitis. Our previous studies confirmed ALI shown by increased WBCs, IFN-γ and TGF-β levels, oxidant/antioxidant imbalance, reduced level of IL-4 in the BALF, and induced lung pathological changes, as well as systemic inflammation by increased numbers of WBC (total and differential) count, and oxidative stress markers, but reduced antioxidant markers in the serum of the mice following chronic systemic administration of LPS.21,25-27 The above studies support the results of the present study regarding LPS-induced ALI and systemic inflammation. Significant correlations between the BALF and blood numbers of WBC (total and differential) may suggest a link between the ALI and systemic inflammation. Therefore, systemic administration of LPS perhaps induces systemic inflammation and oxidative stress and these changes in turn may induce ALI.
In the saline-treated groups, Los and GW9662 did not affect systemic or lung inflammation parameters. These results indicated that these two agents do not have a modulatory effect on the immune system or oxidative stress markers of healthy animals.
The present findings also indicate that treatment with Los improves the systemic and pulmonary complications induced by LPS exposure. Administration of Los significantly reduced the blood numbers of WBC (total and differential), and improved oxidant/antioxidant balance in the serum, indicating the protective effect of Los against LPS-induced systemic oxidative stress and inflammation. The numbers of WBC (total and differential), the levels of IL-4, IFN-γ, and TGF-β and INF-γ/IL-4 ratio in the BALF as well as lung pathological changes were also improved by Los treatment similarly indicating its therapeutic effects on LPS-induced ALI. In contrast, treatment with GW9662 had no effect on inflammatory or oxidative parameters in the blood or the BALF.
In the previous studies, administration of Los abolished the angiotensin enhanced endothelin-1-induced bovine bronchi contractions, an effect which was mediated via an angiotensin II receptor type 2 receptor (AT2R),28 and improved ALI by decreasing NF-kβ activity, synthesis of TNF-α and apoptosis as well as lung pathological changes.29 Los significantly diminished TNF-α in the BALF, myeloperoxidase (MPO) activity in the lung tissues, intercellular adhesion molecule-1 (ICAM-1), caspase-3, lung pathological changes, inflammation and cell apoptosis in a rat model of ALI.30 Los prevented high volume ventilation-caused ALI via reducing BALF total protein, MPO, neutrophil infiltration and pathological changes.31 In addition ALI induced by sepsis also improved by Los through reducing NF-Kβ activation and mitogen-activated protein kinases, as well as the LPS + ATP-induced production of IL-1β protein in the mouse macrophage induced NALP3 inflammasome activation.32 The inhibitory effect of angiotensin II receptor blockers on ROS production via the blockade of the AT1 receptor was also reported.33,34 The studies mentioned above reinforce the findings of this research, highlighting Los protective role in preventing ALI and mitigating systemic inflammation and oxidative stress caused by systemic LPS administration.
The results of this study showed that the effects of treatment with GW-Los combination on improvement of lymphocyte and eosinophil count in the blood and BALF, serum antioxidants, and BALF levels of IL-4, IFN-γ and TGF-β as well as lung pathological changes including emphysema, interstitial inflammation and lymphoid infiltration were lower than the effects of Los treatment. These results indicated that the effects of Los were partially abolished by GW9662 as a PPARγ-receptor antagonist drug and suggest that Los probably suppresses inflammatory process via a PPARγ-receptor dependent mechanism.
GW9662, as a selective PPARγ antagonist, reduced the effects of Los, demonstrating that PPARγ activation is contribute losartan’s amelioration of lung and systemic inflammation induced by LPS.
In human THP-1 macrophages, Los exhibited preventive effects against LPS-induced upregulation of pro-inflammatory genes by activating the PPARγ. Specifically, when THP-1 macrophages are stimulated with LPS, they typically increase the expression of pro-inflammatory cytokines such as TNF-α, IL-6, and IL-1β, contributing to the inflammatory response. Los, an angiotensin II receptor blocker, has been shown to activate PPARγ, a nuclear receptor that plays a key role in regulating inflammation. Activation of PPARγ by Los leads to the transcriptional repression of these pro-inflammatory genes, thereby reducing the production of inflammatory cytokines. This mechanism attenuate the inflammatory response induced by LPS in macrophages, suggesting a potential anti-inflammatory role for Los beyond its cardiovascular effects.35 Treatment with Los also reduced the risk of the liver injury induced by ischemia/reperfusion injury through activation of PPAR-γ receptor.36 It was also shown that EXP3179, an active Los metabolite, acts as a partial PPAR-γ agonist.37 The inhibitory effect of EXP3179 on the endothelial cyclooxygenase (COX)-2 expression and its potent anti-inflammatory effect was also indicated.38 Anti-inflammatory property of ligand-activated PPAR-γ was induced by suppressing pro-inflammatory transcription factors including NF- κB and AP-1.39 Inhibitory effect of COX-2 promoter and mRNA by PPAR-γ receptor activation via interacting with the c-jun component of the AP-1 complex was also shown.40 Studies indicate that Los can up-regulate PPARγ expression, which in turn represses pathways such as TGF-β1, further contributing to lung protection and reducing lung fibrosis.41 Research in other organs (liver, kidney) has shown that Los protective effects are diminished when PPARγ is antagonized; supporting the idea, that PPARγ activation is a key mediator of Los tissue-protective actions.42,43 While much of this evidence comes from hepatic and renal models, the mechanisms are relevant to lung injury as well, given the shared pathways of inflammation and oxidative stress. These studies support the findings of the present study that anti-inflammatory effects of Los is mediated at list in part, mediated through PPAR-γ receptor activation. PPARγ activation is known to suppress the production of pro-inflammatory cytokines and inhibit inflammatory signaling pathways, such as NF-κB, which are central to LPS-induced lung injury.42-44 By activating PPARγ, Los can reduce the inflammatory response in lung tissues. PPARγ enhances cellular antioxidant systems, thereby reducing oxidative stress, a major factor in tissue damage during ALI.42,43 Los activation of PPARγ protect lung cells from oxidative damage was shown in this study. However in further studies the effect of higher doses of GW9662 on LPS-induced systemic and lung inflammation should be examined. In addition, examining the effect of labeled Los on PPARγ receptor and detailed molecular pathway analysis also could be performed in further studies.
Conclusion
These findings demonstrated that Los as an angiotensin receptor inhibitor is able to prevent ALI as well as systemic inflammation and oxidative stress induced by LPS in mice but activation of the PPARγ receptors only partially contribute to this effect.
Competing Interests
The authors declare that they have no conflict of interest.
Data Availability Statement
Data will be made available on request.
Ethical Approval
For the care and use of animals, all applicable international, national, and/or institutional guidelines were followed.
References
- Parikh R, Shah TG, Tandon R. COPD exacerbation care bundle improves standard of care, length of stay, and readmission rates. Int J Chron Obstruct Pulmon Dis 2016; 11:577-83. doi: 10.2147/copd.S100401 [Crossref] [ Google Scholar]
- Tashkin DP, Murray RP. Smoking cessation in chronic obstructive pulmonary disease. Respir Med 2009; 103(7):963-74. doi: 10.1016/j.rmed.2009.02.013 [Crossref] [ Google Scholar]
- Takizawa H, Tanaka M, Takami K, Ohtoshi T, Ito K, Satoh M. Increased expression of inflammatory mediators in small-airway epithelium from tobacco smokers. Am J Physiol Lung Cell Mol Physiol 2000; 278(5):L906-13. doi: 10.1152/ajplung.2000.278.5.L906 [Crossref] [ Google Scholar]
- Mills PR, Davies RJ, Devalia JL. Airway epithelial cells, cytokines, and pollutants. Am J Respir Crit Care Med 1999; 160(5 Pt 2):S38-43. doi: 10.1164/ajrccm.160.supplement_1.11 [Crossref] [ Google Scholar]
- Hellermann GR, Nagy SB, Kong X, Lockey RF, Mohapatra SS. Mechanism of cigarette smoke condensate-induced acute inflammatory response in human bronchial epithelial cells. Respir Res 2002; 3(1):22. doi: 10.1186/rr172 [Crossref] [ Google Scholar]
- Takizawa H, Tanaka M, Takami K, Ohtoshi T, Ito K, Satoh M. Increased expression of transforming growth factor-beta1 in small airway epithelium from tobacco smokers and patients with chronic obstructive pulmonary disease (COPD). Am J Respir Crit Care Med 2001; 163(6):1476-83. doi: 10.1164/ajrccm.163.6.9908135 [Crossref] [ Google Scholar]
- Li Y, Huang J, Foley NM, Xu Y, Li YP, Pan J. B7H3 ameliorates LPS-induced acute lung injury via attenuation of neutrophil migration and infiltration. Sci Rep 2016; 6:31284. doi: 10.1038/srep31284 [Crossref] [ Google Scholar]
- Meyer PW, Ally M, Tikly M, Tintinger G, Winchow LL, Steel H. Tobacco-derived lipopolysaccharide, not microbial translocation, as a potential contributor to the pathogenesis of rheumatoid arthritis. Mediators Inflamm 2019; 2019:4693870. doi: 10.1155/2019/4693870 [Crossref] [ Google Scholar]
- Niehaus I, Lange JH. Endotoxin: is it an environmental factor in the cause of Parkinson’s disease?. Occup Environ Med 2003; 60(5):378. doi: 10.1136/oem.60.5.378 [Crossref] [ Google Scholar]
- Lee WL, Downey GP. Neutrophil activation and acute lung injury. Curr Opin Crit Care 2001; 7(1):1-7. doi: 10.1097/00075198-200102000-00001 [Crossref] [ Google Scholar]
- Zeng M, Sang W, Chen S, Chen R, Zhang H, Xue F. 4-PBA inhibits LPS-induced inflammation through regulating ER stress and autophagy in acute lung injury models. Toxicol Lett 2017; 271:26-37. doi: 10.1016/j.toxlet.2017.02.023 [Crossref] [ Google Scholar]
- Tang R, Pei L, Bai T, Wang J. Down-regulation of microRNA-126-5p contributes to overexpression of VEGFA in lipopolysaccharide-induced acute lung injury. Biotechnol Lett 2016; 38(8):1277-84. doi: 10.1007/s10529-016-2107-2 [Crossref] [ Google Scholar]
- Dong ZW, Yuan YF. Juglanin suppresses fibrosis and inflammation response caused by LPS in acute lung injury. Int J Mol Med 2018; 41(6):3353-65. doi: 10.3892/ijmm.2018.3554 [Crossref] [ Google Scholar]
- Wang Y, Chen J, Chen W, Liu L, Dong M, Ji J. LINC00987 ameliorates COPD by regulating LPS-induced cell apoptosis, oxidative stress, inflammation and autophagy through Let-7b-5p/SIRT1 axis. Int J Chron Obstruct Pulmon Dis 2020; 15:3213-25. doi: 10.2147/copd.S276429 [Crossref] [ Google Scholar]
- Søyseth V, Brekke PH, Smith P, Omland T. Statin use is associated with reduced mortality in COPD. Eur Respir J 2007; 29(2):279-83. doi: 10.1183/09031936.00106406 [Crossref] [ Google Scholar]
- Paulin P, Maritano Furcada J, Ungaro CM, Bendelman G, Waisman GD, Castro HM. Effect of angiotensin 2 receptor blockers on chronic obstructive lung disease mortality: a retrospective cohort study. Pulm Pharmacol Ther 2017; 44:78-82. doi: 10.1016/j.pupt.2017.03.007 [Crossref] [ Google Scholar]
- Mancini GB, Etminan M, Zhang B, Levesque LE, FitzGerald JM, Brophy JM. Reduction of morbidity and mortality by statins, angiotensin-converting enzyme inhibitors, and angiotensin receptor blockers in patients with chronic obstructive pulmonary disease. J Am Coll Cardiol 2006; 47(12):2554-60. doi: 10.1016/j.jacc.2006.04.039 [Crossref] [ Google Scholar]
- Keddissi JI, Younis WG, Chbeir EA, Daher NN, Dernaika TA, Kinasewitz GT. The use of statins and lung function in current and former smokers. Chest 2007; 132(6):1764-71. doi: 10.1378/chest.07-0298 [Crossref] [ Google Scholar]
- Sokar SS, Afify EH, Osman EY. Dexamethasone and losartan combination treatment protected cigarette smoke-induced COPD in rats. Hum Exp Toxicol 2021; 40(2):284-96. doi: 10.1177/0960327120950012 [Crossref] [ Google Scholar]
- Abd El Fattah MA, Abdelhamid YA, Elyamany MF, Badary OA, Heikal OA. Rice bran extract protected against LPS-induced neuroinflammation in mice through targeting PPAR-γ nuclear receptor. Mol Neurobiol 2021; 58(4):1504-16. doi: 10.1007/s12035-020-02196-7 [Crossref] [ Google Scholar]
- Saadat S, Beheshti F, Askari VR, Hosseini M, Mohamadian Roshan N, Boskabady MH. Aminoguanidine affects systemic and lung inflammation induced by lipopolysaccharide in rats. Respir Res 2019; 20(1):96. doi: 10.1186/s12931-019-1054-6 [Crossref] [ Google Scholar]
- Salmani H, Hosseini M, Beheshti F, Baghcheghi Y, Sadeghnia HR, Soukhtanloo M. Angiotensin receptor blocker, losartan ameliorates neuroinflammation and behavioral consequences of lipopolysaccharide injection. Life Sci 2018; 203:161-70. doi: 10.1016/j.lfs.2018.04.033 [Crossref] [ Google Scholar]
- Shakeri F, Soukhtanloo M, Boskabady MH. The effect of hydro-ethanolic extract of Curcuma longa rhizome and curcumin on total and differential WBC and serum oxidant, antioxidant biomarkers in rat model of asthma. Iran J Basic Med Sci 2017; 20(2):155-65. doi: 10.22038/ijbms.2017.8241 [Crossref] [ Google Scholar]
- Boskabady MH, Tabatabaee A, Jalali S. Potential effect of the extract of Zataria multiflora and its constituent, carvacrol, on lung pathology, total and differential WBC, IgE and eosinophil peroxidase levels in sensitized guinea pigs. J Funct Foods 2014; 11:49-61. doi: 10.1016/j.jff.2014.08.021 [Crossref] [ Google Scholar]
- Boskabadi J, Askari VR, Hosseini M, Boskabady MH. Immunomodulatory properties of captopril, an ACE inhibitor, on LPS-induced lung inflammation and fibrosis as well as oxidative stress. Inflammopharmacology 2019; 27(3):639-47. doi: 10.1007/s10787-018-0535-4 [Crossref] [ Google Scholar]
- Boskabadi J, Mokhtari-Zaer A, Abareshi A, Khazdair MR, Emami B, Mohammadian Roshan N. The effect of captopril on lipopolysaccharide-induced lung inflammation. Exp Lung Res 2018; 44(4-5):191-200. doi: 10.1080/01902148.2018.1473530 [Crossref] [ Google Scholar]
- Mokhtari-Zaer A, Norouzi F, Askari VR, Khazdair MR, Mohammadian Roshan N, Boskabady M. The protective effect of Nigella sativa extract on lung inflammation and oxidative stress induced by lipopolysaccharide in rats. J Ethnopharmacol 2020; 253:112653. doi: 10.1016/j.jep.2020.112653 [Crossref] [ Google Scholar]
- Nally JE, Clayton RA, Wakelam MJ, Thomson NC, McGrath JC. Angiotensin II enhances responses to endothelin-1 in bovine bronchial smooth muscle. Pulm Pharmacol 1994; 7(6):409-13. doi: 10.1006/pulp.1994.1048 [Crossref] [ Google Scholar]
- Liu L, Qiu HB, Yang Y, Wang L, Ding HM, Li HP. Losartan, an antagonist of AT1 receptor for angiotensin II, attenuates lipopolysaccharide-induced acute lung injury in rat. Arch Biochem Biophys 2009; 481(1):131-6. doi: 10.1016/j.abb.2008.09.019 [Crossref] [ Google Scholar]
- Deng W, Deng Y, Deng J, Wang DX, Zhang T. Losartan attenuated lipopolysaccharide-induced lung injury by suppression of lectin-like oxidized low-density lipoprotein receptor-1. Int J Clin Exp Pathol 2015; 8(12):15670-6. [ Google Scholar]
- Shen L, Mo H, Cai L, Kong T, Zheng W, Ye J. Losartan prevents sepsis-induced acute lung injury and decreases activation of nuclear factor kappaB and mitogen-activated protein kinases. Shock 2009; 31(5):500-6. doi: 10.1097/SHK.0b013e318189017a [Crossref] [ Google Scholar]
- Wang F, Huang L, Peng ZZ, Tang YT, Lu MM, Peng Y. Losartan inhibits LPS + ATP-induced IL-1beta secretion from mouse primary macrophages by suppressing NALP3 inflammasome. Pharmazie 2014; 69(9):680-4. [ Google Scholar]
- Ogawa S, Mori T, Nako K, Kato T, Takeuchi K, Ito S. Angiotensin II type 1 receptor blockers reduce urinary oxidative stress markers in hypertensive diabetic nephropathy. Hypertension 2006; 47(4):699-705. doi: 10.1161/01.HYP.0000203826.15076.4b [Crossref] [ Google Scholar]
- Satoh M, Fujimoto S, Arakawa S, Yada T, Namikoshi T, Haruna Y. Angiotensin II type 1 receptor blocker ameliorates uncoupled endothelial nitric oxide synthase in rats with experimental diabetic nephropathy. Nephrol Dial Transplant 2008; 23(12):3806-13. doi: 10.1093/ndt/gfn357 [Crossref] [ Google Scholar]
- Jafri SH, Glass J, Shi R, Zhang S, Prince M, Kleiner-Hancock H. Thymoquinone and cisplatin as a therapeutic combination in lung cancer: In vitro and in vivo. J Exp Clin Cancer Res 2010; 29(1):87. doi: 10.1186/1756-9966-29-87 [Crossref] [ Google Scholar]
- Koh EJ, Yoon SJ, Lee SM. Losartan protects liver against ischaemia/reperfusion injury through PPAR-γ activation and receptor for advanced glycation end-products down-regulation. Br J Pharmacol 2013; 169(6):1404-16. doi: 10.1111/bph.12229 [Crossref] [ Google Scholar]
- Schupp M, Lee LD, Frost N, Umbreen S, Schmidt B, Unger T. Regulation of peroxisome proliferator-activated receptor gamma activity by losartan metabolites. Hypertension 2006; 47(3):586-9. doi: 10.1161/01.HYP.0000196946.79674.8b [Crossref] [ Google Scholar]
- Krämer C, Sunkomat J, Witte J, Luchtefeld M, Walden M, Schmidt B. Angiotensin II receptor-independent antiinflammatory and antiaggregatory properties of losartan: role of the active metabolite EXP3179. Circ Res 2002; 90(7):770-6. doi: 10.1161/01.res.0000014434.48463.35 [Crossref] [ Google Scholar]
- Pascual G, Fong AL, Ogawa S, Gamliel A, Li AC, Perissi V. A SUMOylation-dependent pathway mediates transrepression of inflammatory response genes by PPAR-gamma. Nature 2005; 437(7059):759-63. doi: 10.1038/nature03988 [Crossref] [ Google Scholar]
- Subbaramaiah K, Lin DT, Hart JC, Dannenberg AJ. Peroxisome proliferator-activated receptor gamma ligands suppress the transcriptional activation of cyclooxygenase-2 Evidence for involvement of activator protein-1 and CREB-binding protein/p300. J Biol Chem 2001; 276(15):12440-8. doi: 10.1074/jbc.M007237200 [Crossref] [ Google Scholar]
- Deng Z, Chen F, Liu Y, Wang J, Lu W, Jiang W. Losartan protects against osteoarthritis by repressing the TGF-β1 signaling pathway via upregulation of PPARγ. J Orthop Translat 2021; 29:30-41. doi: 10.1016/j.jot.2021.03.005 [Crossref] [ Google Scholar]
- Huang R, Zhang C, Wang X, Hu H. PPARγ in ischemia-reperfusion injury: overview of the biology and therapy. Front Pharmacol 2021; 12:600618. doi: 10.3389/fphar.2021.600618 [Crossref] [ Google Scholar]
- Saravi B, Li Z, Pfannkuche J, Wystrach L, Häckel S, E E. Albers C, et al Angiotensin II type 1 receptor antagonist losartan inhibits TNF-α-induced inflammation and degeneration processes in human nucleus pulposus cells. Appl Sci 2021; 11(1):417. doi: 10.3390/app11010417 [Crossref] [ Google Scholar]
- Şahin S, Aydın A, Göçmen AY, Kaymak E. Evaluation of the protective effect of losartan in acetaminophen-induced liver and kidney damage in mice. Naunyn Schmiedebergs Arch Pharmacol 2024; 397(7):5067-78. doi: 10.1007/s00210-023-02937-0 [Crossref] [ Google Scholar]