Pharmaceutical Sciences. 31(4):497-505.
doi: 10.34172/PS.025.42320
Research Article
Evaluation of the Effect of the Oral Formulation Prepared from the Extract of Pomegranate Peel for the Treatment of Benign Prostate Hyperplasia: A Triple-Blind Randomized Clinical Trial
Mehrshad Ebrahimpour Investigation, Visualization, Writing – original draft, Writing – review & editing, 1 
Javad Darabi Mahboub Formal analysis, Investigation, Validation, Writing – review & editing, 1
Melika Ahmadi Investigation, 1
Samin Ghorbani Moghadam Visualization, Writing – original draft, Writing – review & editing, 1
Mohammad Reza Darabi Mahboub Conceptualization, Methodology, Supervision, Writing – review & editing, 2
Alireza Akhavan Rezayat Conceptualization, Methodology, Supervision, Writing – review & editing, 2
Sepideh Elyasi Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Project administration, Resources, Software, Supervision, Validation, Writing – review & editing, 3, *
Author information:
1School of Pharmacy, Mashhad University of Medical Sciences, Mashhad, Iran
2Department of Urology, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran
3Department of Clinical Pharmacy, School of Pharmacy, Mashhad University of Medical Sciences, Mashhad, Iran
Abstract
Background:
Benign prostatic hyperplasia (BPH) is a common condition affecting older men, primarily driven by hormonal imbalances and inflammation. This study aimed to investigate the effects of pomegranate peel extract, rich in anti-inflammatory and antioxidant polyphenolic compounds like anthocyanins and tannins, on BPH symptoms compared to a placebo.
Methods:
Forty patients aged 50-80 with BPH from Ghaem Hospital in Mashhad were randomly assigned to either the treatment or control group. The treatment group (20 patients) received 250 mg of pomegranate peel extract capsules three times daily alongside tamsulosin 0.4 mg nightly for four months. In the control group (20 patients) lactose capsules was prescribed as a placebo with the same dosing. The severity of lower urinary symptoms was assessed using the International Prostate Symptom Score (IPSS), along with prostate size via ultrasound at baseline and after 2 and 4 months and prostate-specific antigen (PSA) serum levels just at the beginning and end of study.
Results:
Baseline prostate sizes, PSA serum level and IPSS scores were comparable between two groups (P>0.05). At the 4-month follow-up, the pomegranate peel extract group demonstrated significantly lower symptom scores compared to the placebo group (P=0.004), although no meaningful difference was observed after 2 months (P=0.067). Moreover, the prostate size did not change meaningfully after 2 and 4 months in comparison with the placebo group (P=0.226 & 0.355) and also PSA serum level was not significantly lower in pomegranate group after 4 months of therapy (P=206).
Conclusion:
As indicated by the IPSS, a daily regimen of 250 mg of pomegranate peel extract for four months effectively alleviated BPH symptoms. This suggests its potential as a treatment option for BPH, warranting further human studies to explore its efficacy.
Keywords: Benign prostatic hyperplasia, BPH, Pomegranate
Copyright and License Information
© 2025 The Author(s).
This is an open access article and applies the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
This study was supported by Mashhad University of Medical Sciences, Mashhad, Iran.
Introduction
Benign prostatic hyperplasia (BPH) is a prevalent disease that affects nearly 105 million men worldwide. Approximately half of all men have BPH by the time they are 50 years old. The condition usually first manifests after the age of 40. The incidence is still increasing, with men over 80 years old having a prevalence of up to 90%.1,2 The main feature of BPH is the growth of the prostate gland; nevertheless, this is neither a sign nor a precursor to prostate cancer.3 Prostate-specific antigen (PSA) levels in men with BPH may be raised, although there is no correlation between this disease and a higher risk of prostate cancer.
The most prevalent cause of lower urinary tract symptoms (LUTS), is BPH. These symptoms may be accompanied by bladder pain or dysuria.4-6 Bladder outlet obstruction can also result from BPH.7 BPH is a progressive disease that elevates the possibility of urinary tract infections if left untreated. It may additionally result in incomplete bladder emptying, which can leave residual urine or urine stasis.8
Etiology of BPH is yet unclear. Nonetheless, it seems that several circumstances had a substantial impact on the emergence of this illness.
Experts generally agree that androgens are important in the pathophysiology of BPH. However, empirical research indicates that while androgens are necessary, they are not sufficient for the initiation of BPH. Estrogen might also play a role in the development of BPH, possibly utilizing the local transformation of androgens to estrogen in the prostatic tissue.9
Based on the location inside the prostate (the TZ) that BPH affects, we hypothesize that years of exposure to the urinary toxins that particularly appear in ageing and obese men play the main rule in disruption of tissue homeostasis in the TZ which results in the onset of BPH. As is the case of BPH progression, it is clear that the nodular hyperplasia in either stroma or epithelium or both is promoted by a cascade of cellular responses to the molecular events of intraprostatic DHT, chronic inflammation, E2, and perhaps other growth factors (eg, PEDF) from the testicles.10
The available data points to the possibility that the pathophysiology of BPH may involve both acute and chronic inflammation. Through some processes, inflammation appears to promote the growth of cells, most notably by causing oxidative stress. The onset and course of BPH may be impacted by this inflammatory process.11
This condition is treated with a variety of methods, such as changes to lifestyle variables, medications, and different procedural and surgical techniques. The existing data, however limited, indicates that weight control by dietary change, improved physical activity, and decreased caffeine use may be helpful for patients presenting with mild symptoms who are at the beginning of the disease12,13 The pharmacological treatments could involve the use of alpha-blockers like terazosin and tamsulosin or 5-alpha-reductase inhibitors like finasteride and beta-3 adrenergic agonists. Surgery to remove a piece of the prostate gland may be performed if conservative approaches are unsuccessful. Alpha-adrenergic receptor blockers are used as initial pharmacologic agents in most patients. They reduce symptoms effectively within days and are well tolerated. However, blood pressure should be monitored at the beginning of treatment due to the risk of hypotension; but the risk is higher with terazosin and doxazosin in comparison with tamsulosin. For patients with an estimated prostate size above 30 g, a 5-alpha-reductase inhibitor (5-ARI) is added to reduce stimulation of the prostate.14 However, there are some concerns regarding high-grade prostate cancer.15,16 Moreover, sexual dysfunction, including erectile dysfunction, ejaculatory dysfunction or decreased libido are common with 5-ARI, which may even continue after discontinuation of the medication (post-finasteride syndrome).17,18 While these therapies reduce the risk of symptomatic progression by 30%–40% 19 beside abovementioned adverse reactions, there is a considerable need for more effective and safe treatments at least an adjuvant measure.
So, the use of herbal medicines, such as saw palmetto, has been examined as an additional therapeutic strategy; nevertheless, there is still a dearth of empirical data to support their effectiveness. Other herbal therapies that have been used to treat this illness include beta-sitosterol obtained from Hypoxis rooperi, pygeum extracted from Prunus africana bark, Cucurbita pepo seed, and Urtica dioica root.20-22 in a European survey, phytotherapy was the second most commonly prescribed remedy beside alpha-adrenergic blocker monotherapy.23
Pomegranate (Punica granatum) is another plant that has been investigated concerning the treatment of BPH. The Punicaceae family includes the genus Punica, which includes pomegranates. This plant has considerable anti-inflammatory qualities, which are explained by its ability to inhibit the enzymes lipoxygenase (LOX) and cyclooxygenase (COX).24 In addition, pomegranate juice’s polyphenolic components have strong antioxidant and antiangiogenic properties.25,26 Furthermore, observations from preclinical and clinical studies have indicated that pomegranate juice inhibits cell proliferation.27 Pomegranate juice has also been shown in other research to elicit pro-apoptotic effects and to block cell cycle progression in breast cancer, colon cancer, and the prostate cancer cell line PC3.28,29 In a clinical trial, men who had undergone surgical or radiation therapy for prostate cancer and subsequently received 8 ounces of pomegranate juice (equivalent to 570 mg of gallic acid) exhibited a prolonged time to PSA doubling, increasing from an average of 15 months to 54 months. Additionally, in vitro studies have revealed a 17% increase in cell apoptosis, a 12% decrease in cell proliferation, and a significant reduction in oxidative stress.30
The rationale for utilizing pomegranate peel extract lies in the observation that its concentrations of phenolics, flavonoids, and proanthocyanidins are higher compared to those in pomegranate pulp extract.31 The predominant phytochemicals in pomegranate peel extract are polyphenols, particularly hydrolyzable tannins known as ellagitannins. Furthermore, pomegranate peel extract contains substantial quantities of condensed tannins, catechin, and prodelphinidin, which are present in greater amounts than those found in pomegranate juice.25-27 Moreover, utilizing the peel as the active ingredient would be a more cost-effective approach. Additionally, this approach would help to reduce waste and promote environmental sustainability by utilizing the otherwise discarded pomegranate peel.
The aim of this study is to evaluate the oral formulation of pomegranate peel extract for the management of BPH as an adjuvant treatment besides tamsulosin.
Material and Methods
Study design
This study was a triple-blind, randomized, placebo-controlled clinical trial assessing the effect of the oral formulation prepared from the extract of pomegranate peel for the treatment of BPH that was conducted from June 2021 to January 2023 at the Ghaem Hospital affiliated with Mashhad University of Medical Sciences, Mashhad, Iran.
Study population
The eligibility criteria for the study were as follows: male patients between the ages of 50 and 80 years, with a clinical diagnosis of BPH; Specifically, the participants were required to have LUTS and signing the informed consent form. Patients were not included the following conditions: 1) Concurrent use of BPH medications other than tamsulosin. 2) Consumption of supplements for BPH, such as vitamin E, saw palmetto, and quercetin. 3) Presence of prostate or bladder cancer. 4) History of prostate surgery. 5) PSA level greater than 4 mg/ml. 6) History of sensitivity to pomegranate or its derivatives. 7) Use of drugs with significant metabolism by the CYP3A4 enzyme. 8) Current active urinary tract infection or bladder stone. Patients were excluded from the study in case of the occurrence of significant systolic or diastolic blood pressure drop upon taking the study medication, considerable consumption of pomegranate or pomegranate juice by the participant, patient’s refusal to continue participating in the study and occurrence of severe constipation or hemorrhoids during treatment that cannot be controlled with simple medical measures.
Study protocols
In this research, 40 individuals with BPH who were between the ages of 50 and 80 were selected from the outpatient clinic of Ghaem Hospital, Mashhad, Iran. Patients were randomly assigned to either medication or the placebo group at a 1:1 ratio.
Patients in the medication intervention group (n = 20) were given tamsulosin capsule 0.4 mg every night in addition to one capsule containing 250 mg of pomegranate peel whole extract three times a day, for four months. The placebo group (n = 20) was given placebo capsules. The lactose-containing placebo capsules were made to resemble pharmaceutical capsules. It should be mentioned that in all included patients tamsulosin capsule was also prescribed just concurrently with the pomegranate or placebo capsules and they were tamsulosin naïve.
As human studies have yet to assess the efficacy of pomegranate compounds in BPH, the only available animal study involving rats was utilized to establish pomegranate dose for the current study. It is recommended that, in the absence of human studies, an initial dose ranging from one-tenth to one-hundredth of the animal dose be applied in human trials.32 Given the animal study’s dosage of 100 mg/kg, applying the one-tenth rule results in a calculated dose of 750 mg for an average individual weighing 75 kg. Additionally, based on the analysis of ellagic acid content in the pomegranate peel extract by using high-performance liquid chromatography (HPLC) method, it was determined to be 2.2%. According to available data, the minimum effective blood concentration of ellagic acid is approximately 14 mg.33 Therefore, this minimum concentration can be achieved with the specified dosage, given the 2.2% content of ellagic acid.33
In this study, the pomegranate peel extract was obtained from Rezvan DanehTM Company, Kashmar, Iran. The alginic acid content of the extract and the quality of the powder were determined HPLC analysis conducted in the laboratory of the Golexir ParsTM Company.
During the trial, patients were advised not to consume over-the-counter pharmaceuticals, herbal therapies, or any additional prescribed medication for the management of BPH. If such supplementary drug usage transpires, the patient would be excluded from the research.
Outcomes
All patients were evaluated by urologist and the pharmacist regarding the completion of the inclusion criteria at the beginning of the study. Patients’ demographic data, past medical and drug history were recorded at the beginning of the study. Additionally, the IPSS criteria were used to determine the initial level of severity of the patient’s LUTS. Prostate size and serum PSA levels were also documented. Every two months, the study team and attending physician used the IPSS criteria to evaluate the progress of the condition, as the primary outcome. During these follow-up visits, measurements and records of the prostate size and serum PSA levels were also collected, as the secondary outcomes.
The participants were also continuously observed for any adverse events, including disorientation, blood pressure variations, postural hypotension, gastrointestinal adverse reactions and other possible side effects.
Patient follow-up
The patients were also monitored in terms of their compliance with the prescribed treatment. Adherence to the treatment was determined based on whether the patients consumed more than 80% of the recommended capsules.
Sample size
Given the lack of prior human studies evaluating the effectiveness of pomegranate peel extract in the treatment of BPH, the present study can be considered a pilot investigation. Based on Whitehead et al recommendation, for a main trial designed with 90% power and two-sided 5% significance, pilot trial sample sizes per treatment arm of 75, 25, 15 and 10 is enough for standardized effect sizes that are extra small ( ≤ 0.1), small (0.2), medium (0.5) or large (0.8), respectively.34 So, proposing the pomegranate peel extract effect small to medium, 15-25 patients in each arm could be acceptable and we defined the sample size 20 patients in each arm.
Randomization and blinding
The pharmaceutical laboratory of the Mashhad Faculty of Pharmacy developed and packaged the medication and placebo formulations. Patients were randomly allocated to each group using block randomization with blocks of size four (10 block of size four). A computer-generated randomization list obtained from Randomization.com. To secure the study under a blind condition, pomegranate and placebo tablets were packed in boxes with the same shape and size labeled with numbers from 1 to 40, based on the prepared randomization list by the laboratory personnel who did not involve in patient selection and assessment process. Each patient who has fulfilled the entry criteria received a box with number 1 to 40, containing either a pomegranate or a placebo, respectively by the urologist. Patients were assessed during the study by the urologist and pharmacist. The pharmacist carried out the data collection and the clinical pharmacist analyzed the data which was inserted to the SPSS file by the pharmacist, defining the treatment or placebo by letter A or B to keep the analyzer blind. This approach was employed to maintain the integrity of the triple-blind, placebo-controlled study design, where neither the participants nor the treating physician evaluating the outcomes were aware of the specific treatment received by each participant. Besides, the analyzer was also blind and the groups were presented in the SPSS file with A/B code and these codes were defined just after the end of analysis. This blinding process helped to minimize potential biases and ensure the objectivity of the study findings.
Statistical methods
The statistical analyses were performed using SPSS version 25 software. For the comparison of quantitative variables between the treatment groups before and after the intervention, we used the independent sample t-test for data with a normal distribution and the Mann-Whitney test for data with a non-normal distribution. For the comparison of qualitative variables between the groups, Fisher’s exact test was employed. To evaluate the intra-group changes over time, we used the repeated measures test for data with a normal distribution, and the Friedman test for data with a non-normal distribution. The significance level for all statistical tests was set at a P value less than 0.05.
Results
Baseline characteristics and laboratory data of the study population
Initially, 59 people were recruited for the study. A total sample size of 40 individuals was achieved after 19 participants were eliminated during the investigation (Figure 1). The subjects were split into two groups at random: twenty patients were given pomegranate peel extract, and the other twenty were given capsules containing a placebo.
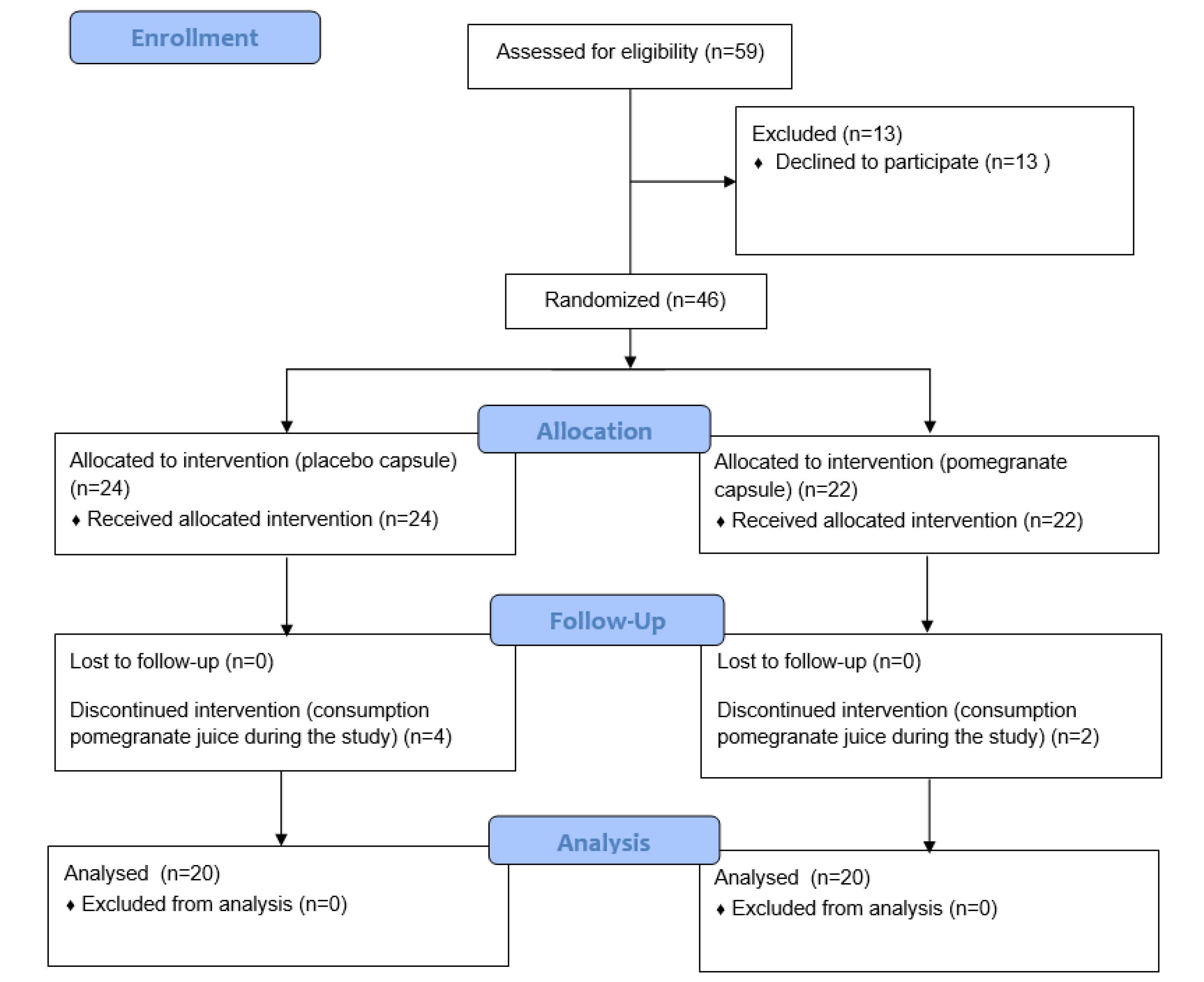
Figure 1.
CONSORT subject flow diagram shows the number of subjects screened, enrolled, randomized, and included in the study
.
CONSORT subject flow diagram shows the number of subjects screened, enrolled, randomized, and included in the study
The average age of the participants in the trial was 64.9 ± 6.1 years, whereas the mean age of the pomegranate capsule group was 64.3 ± 4.1 years and that of the placebo group was 65.4 ± 5.2 years. There was no discernible difference in the mean age of the two treatment groups, according to statistical analysis (P = 0.12). Moreover, the past medical history was comparable between two groups and diabetes mellitus was the most common disease in both groups (P = 0.452) (Table 1).
Table 1.
Comparison of baseline characteristics between two groups
|
Variable
|
|
Pomegranate Peel Extract (N=20)
|
Placebo Capsule (N=20)
|
P
value
|
| Age (year) (Mean ± SD) |
|
64.3 ± 4.1 |
65.4 ± 5.2 |
0.1201 |
| Past medical history, n (%) |
Hypertension |
4 (20) |
6 (30) |
0.4522 |
| Diabetes |
6 (30) |
7 (35) |
| Thyroid dysfunction |
2 (10) |
1(5) |
| Psychiatric disease |
3 (15) |
2 (10) |
| Rheumatologic disease |
1(5) |
0 |
| Initial prostate volume (cc) (Mean ± SD) |
|
49.85 ± 11.98 |
56.60 ± 19.73 |
0.2011 |
| Clinical symptoms IPSS score (Median, IQR) |
|
11.5 (7.5–14.75) |
13.5 (9.5–18.5) |
0.1653 |
| Serum PSA level (ng/ml) (Mean ± SD) |
|
1.72 ± 1.61 |
2.11 ± 1.68 |
0.6441 |
1Independent sample T test, 2Chi Square test, 3Mann-Whitney U test.
According to the findings of the clinical symptoms assessment questionnaire, 7 participants (17.5%) exhibited mild symptoms, 27 participants (67.5%) displayed moderate symptoms, and 6 participants (15%) presented with severe symptoms. The mean initial prostate volume was 53.23 ± 16.47 mL. The median score on the patient’s clinical symptom evaluation questionnaire was 13 (IQR = 9-16). There was no significant difference between two groups at the beginning of the study regarding prostate size (P =0.201), clinical symptom score (P = 0.165) and also PSA serum level (P = 0.644).
Clinical characteristics of the study population following the intervention and their intra-group comparisons
After two and four months of treatment, there were no statistically significant differences in prostate volume between the two study groups (P = 0.226 & 0.355, respectively). Besides, a notable reduction in prostate volume was found within the placebo group (P = 0.011), but not in the pomegranate group (P = 0.071) (Table 1).
Based on the data derived from the clinical symptom evaluation questionnaire scores given in Table 2, no significant changes were observed in the group consuming pomegranate peel extract capsules after two months compared to the placebo group (P = 0.067). However, after four months of treatment, the scores for the pomegranate peel extract group were significantly lower (P = 0.004). Additionally, throughout the study, both groups exhibited a notable decrease in their clinical symptom evaluation questionnaire scores (P < 0.001, in both groups).
Table 2.
Comparison of the clinical and laboratory data between two groups during the 4 months follow-up
|
Outcome
|
Time Point
|
Pomegranate Peel Extract (n=20)
|
Placebo (n=20)
|
P
value (between groups)
|
| Prostate volume (mL) (Mean ± SD) |
Baseline |
49.85 ± 11.98 |
56.60 ± 19.73 |
0.2011 |
| After 2 months |
46.95 ± 11.43 |
53.15 ± 19.42 |
0.2261 |
| After 4 months |
45.35 ± 10.81 |
49.25 ± 15.14 |
0.3551 |
|
P value within group2 |
0.071 |
0.011* |
|
| Clinical symptom score (Median, IQR) |
Baseline |
11.5 (7.5–14.75) |
13.5 (9.5–18.5) |
0.1653 |
| After 2 months |
7 (2.5–10.75) |
11.5 (6–14.75) |
0.0673 |
| After 4 months |
4.5 (3–6.75) |
8.5 (5.25–11.75) |
0.0043* |
|
P value within group4 |
< 0.001* |
< 0.001* |
|
| PSA serum level (ng/mL) (Mean ± SD) |
Baseline |
1.72 ± 1.61 |
2.11 ± 1.68 |
0.6441 |
| After 4 months |
1.34 ± 0.67 |
1.65 ± 0.85 |
0.2061 |
1Independent sample T test, 2Repeated measure test, 3Mann-Whitney U test, 4Friedman test.
Considering the PSA serum level, no meaningful difference was found between two groups at the end of the study (P = 0.206) (Table 2).
Besides, comparative analysis of the severity of symptoms between the two study groups after two and four months of treatment just showed significant difference on the second time point (P = 0.321 and 0.008) (Table 2). At the end of study most of patients in the pomegranate group had mild symptoms (85%) but 60% of patients in the placebo group experienced moderate symptoms (Table 3).
Table 3.
A comparative analysis of the severity of symptoms between the two study groups at two distinct time points: two months post-treatment, and four months post-treatment
|
The severity of symptoms
|
Pomegranate peel extract (n=20)
|
Placebo (n=20)
|
P
valuea
|
| After two months of treatment |
| Mild (0-7) |
11 (55%) |
8 (40%) |
0.321 |
| Moderate (8-19) |
8 (40%) |
12 (60%) |
| Severe (20-35) |
1 (5%) |
0 (0%) |
| After four months of treatment |
| Mild (0-7) |
17 (85%) |
8 (40%) |
0.008* |
| Moderate (8-19) |
3 (15%) |
12 (60%) |
| Severe (20-35) |
0 (0%) |
0 (0%) |
Examining the incidence of complications in two treatment groups
No adverse effects associated with the drug were noted or documented in any of the groups receiving either the placebo or the pomegranate peel extract treatment.
Discussion
The current study aimed to assess the efficacy of pomegranate peel extract in alleviating the symptoms associated with BPH. The results revealed that, at the 2-month follow-up, there were no statistically significant differences between the two groups concerning prostate volume, the average scores on the patient symptom evaluation questionnaire, and symptom severity.
At the 4-month follow-up, while no significant differences were found between the groups regarding prostate volume and PSA serum levels, the clinical symptoms evaluation questionnaire scores were notably lower in the group consuming pomegranate peel extract. By the conclusion of the 4 months, the severity of clinical symptoms was significantly reduced in the treatment group. Moreover, although symptom severity decreased in both groups throughout the study, a significant reduction in prostate size was observed solely in the placebo group.
In the present investigation, patients who received pomegranate peel extract exhibited significantly milder clinical symptoms at the 4-month follow-up compared to those in the placebo group, suggesting that pomegranate peel extract may be beneficial during this period. In Sreekumar et al also demonstrated that pomegranate extract was effective in treating prostatic hyperplasia in a mice model. Their results clarified the underlying mechanisms of action, which may have contributed to the observed decrease in symptom severity during the current study’s four months. These mechanisms entail both the induction of apoptosis and the suppression of cell proliferation.35
The research conducted by Consoli et al demonstrated that pomegranate extract significantly enhances the rates of cell proliferation and migration, as well as the clonogenic capacity of BPH-1 cells, while concurrently decreasing levels of inflammatory cytokines and the angiogenic factor, vascular endothelial growth factor- asymmetric dimethylarginine (VEGF-ADMA). Furthermore, this study indicated that pomegranate extract possesses the capability to inhibit angiogenesis in a laboratory model of BPH.26 Also, results consistent with the current study were published by Ammar et al. about the effectiveness of pomegranate extract in reducing testosterone-induced prostate hyperplasia in rats.30
In another investigation, total oxidant status and indicators of oxidative stress were found to be significantly reduced by both the ethanolic and aqueous extracts of pomegranate seeds when administered separately and in combination with dutasteride. As a result, these expected results were supported by the observed benefits of pomegranate peel extract in symptom relief in the current investigation.36
Numerous studies indicate that inflammation may play a role in the development of prostate hyperplasia and its associated symptoms.37 In rodent models, prostatic inflammation has been shown to contribute to the progression of prostatic hyperplasia, while in human subjects, inflammatory infiltrates are frequently observed in prostate tissue samples from men diagnosed with BPH.38,39 Additionally, the presence and severity of inflammation correlate with prostate size, symptom intensity, and an increased risk of acute urinary retention.40-42 Given these findings, it is reasonable to hypothesize that anti-inflammatory agents could mitigate the severity of LUTS related to BPH.
Several studies have demonstrated that pomegranate phytochemicals are effective in reducing oxidative stress and modulating inflammatory pathways. Consequently, the rationale for utilizing pomegranate in the prevention and treatment of BPH is grounded in its influence on the role of inflammation and hypoxia in the pathogenesis of this condition.43
Currently, there is a paucity of clinical trial studies assessing the efficacy of pomegranate extract in the management of BPH. One such clinical trial measured nitric oxide (NO) metabolites to evaluate the antioxidant activity in patients receiving pomegranate extract. After nine months, a significant elevation in serum NO metabolites were observed compared to baseline levels, with two-thirds of the participants exhibiting increased serum NO metabolites.29 This elevation in NO levels appears to play a crucial role in alleviating smooth muscle tension in the lower urinary tract via the NO/cGMP signaling pathway, thereby enhancing hyperplasia-related symptoms. This observation aligns with the symptom improvement noted within four months in the present study.
It is important to note that the majority of prior studies demonstrating the efficacy of pomegranate products on prostate health have monitored treatment outcomes for durations exceeding four months. For instance, the research conducted by Paller et al spanned 18 months, while the study by Thomas et al. lasted for six months.44,45 Consequently, a four-month period may be insufficient to fully assess the effectiveness of pomegranate extracts. Extending the duration of the study could yield different results, potentially explaining the lack of similar findings observed after two months.
In the current study, the prostate volume treated with pomegranate peel extract did not exhibit a statistically significant difference from the placebo in either the two-month or four-month follow-ups. PPE may exert its benefits primarily through anti-inflammatory and antioxidant effects that improve urinary symptoms without causing measurable prostate shrinkage. It seems that PPE’s active compounds do not target pathways that directly reduce prostate tissue mass, like anti-proliferative effects. Another consideration is that prostate size changes may lag behind symptom changes or require longer treatment duration to manifest, so PPE’s symptomatic benefit could precede any size reduction. Further studies could clarify these mechanisms and the time course of prostate size changes.
But the prostate size considerably decreased in the placebo group, in contrast to the treatment group during this 4-month follow-up. Actually, we could not propose any hypothesis for this finding. Our study population in two groups had comparable baseline characteristics, none of them received 5-ARI which could be effective on prostate size and also, they did not use other herbal medication. Dose of tamsulosin was also the same in both groups. May be patients in two groups had difference compliance to tamsulosin, as we did not check it and we just monitored patients’ compliance to the pomegranate/ placebo capsules.
Conversely, previous research by Obisike et al reported a significant reduction in prostate volume in rats following the consumption of pomegranate seeds.46 Similarly, the study by Adhami et al demonstrated a notable effect of pomegranate extract in decreasing prostate volume in the tested mouse subjects.47 It is important to consider that these studies were conducted on animal models, highlighting the necessity for further research involving human subjects to evaluate the impact of pomegranate extract on prostate volume in humans. Moreover, in these two studies pomegranate seed and pomegranate fruit extract were used, but our treatment group received pomegranate peels extract and it may be an influential factor.
Therefore, in conclusion, the insufficient prescribed dose (due to not receiving enough ellagic acid) as well as the short duration of the study can be considered as reasons for the product not being effective in reducing prostate size and PSA serum level.
In the present study, no significant adverse effects were reported among participants consuming pomegranate peel extract. This finding aligns with earlier research conducted by Hikal and Said-Al Ahl, which similarly noted a lack of noteworthy side effects.48 Additionally, the study by Khwairakpam et al indicated that pomegranate extract did not cause any specific adverse effects in cancer patients.49 Furthermore, research by Cheshomi et al found that ellagic acid and other derivatives of pomegranate exhibited no apparent side effects.50
There were some limitations to the present investigation, especially the small sample size. Moreover, estimates from the only available animal study were used to determine the proper dosage of pomegranate peel extract. The relatively short follow-up period is yet another significant study drawback. However, as the strengths of our study, it was the first human study focusing on pomegranate efficacy in management of BPH. Considering its cheap price, promising efficacy of pomegranate peel extract at least in symptomatic alleviation in current study could be used as a basis for further studies.
It is advisable to conduct further research in this domain utilizing a larger sample size and an extended follow-up period within clinical trial methodologies involving human subjects. Additionally, given the demonstrated superior efficacy of pomegranate peel extract over placebo in alleviating the severity of clinical symptoms, it is recommended that future studies investigate the drug’s side effects and optimal dosage. This would make it easier to evaluate the treatment’s advantages and disadvantages thoroughly, which would raise the possibility that pomegranate peel extract will prove to be a useful medical treatment. Additionally, it is recommended that future research compare the efficacy of formulations containing pomegranate peel extract to other complementary herbal products currently on the pharmaceutical market for the treatment of BPH.
Conclusion
The administration of a capsule containing pomegranate peel extract at a dosage of 250 mg three times daily demonstrated greater efficacy than a placebo in mitigating the severity of symptoms associated with prostate hyperplasia over four months. This treatment significantly reduced symptom severity as measured by the IPSS criteria, but not PSA serum level or prostate size. Consequently, it may be regarded as a promising adjuvant treatment for alleviating symptoms of BPH. Further clinical studies involving human subjects on this product are therefore recommended.
Competing Interests
Nothing to declare.
Data Availability Statement
Supporting data will be available based on request.
Ethical Approval
This study was approved by the local Mashhad University of Medical Sciences Ethics Committee (IR.MUMS.REC.1399.132). Also, it has been submitted to the Iranian Registry of Clinical Trials (IRCT20200408046990N4). Additionally, we received consent forms from each participant.
Acknowledgements
The authors appreciate Mashhad University of Medical Sciences for the funding of this research study and Rezvan DanehTM Company, Kashmar, Iran for providing the pomegranate peel extract.
References
- Tavoosian A, Reis LO, Aluru P, Khajavi A, Aghamir SM. Comparison of tamsulosin and tadalafil effects in LUTS treatment considering patients’ atherosclerosis risk level. Ann Med Surg (Lond) 2022; 80:104137. doi: 10.1016/j.amsu.2022.104137 [Crossref] [ Google Scholar]
- Chughtai B, Forde JC, Thomas DD, Laor L, Hossack T, Woo HH. Benign prostatic hyperplasia. Nat Rev Dis Primers 2016; 2:16031. doi: 10.1038/nrdp.2016.31 [Crossref] [ Google Scholar]
- Chang RT, Kirby R, Challacombe BJ. Is there a link between BPH and prostate cancer?. Practitioner 2012; 256(1750):13-6. [ Google Scholar]
- Robinson J. Post-micturition dribble in men: causes and treatment. Nurs Stand 2008; 22(30):43-6. doi: 10.7748/ns2008.04.22.30.43.c6440 [Crossref] [ Google Scholar]
- Sarma AV, Wei JT. Clinical practice Benign prostatic hyperplasia and lower urinary tract symptoms. N Engl J Med 2012; 367(3):248-57. doi: 10.1056/NEJMcp1106637 [Crossref] [ Google Scholar]
- Walker HK, Hall WD, Hurst JW. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd ed. Boston: Butterworths; 1990.
- Dmochowski RR. Bladder outlet obstruction: etiology and evaluation. Rev Urol 2005; 7(Suppl 6):S3-13. [ Google Scholar]
- Truzzi JC, Almeida FM, Nunes EC, Sadi MV. Residual urinary volume and urinary tract infection--when are they linked?. J Urol 2008; 180(1):182-5. doi: 10.1016/j.juro.2008.03.044 [Crossref] [ Google Scholar]
- Ho CK, Nanda J, Chapman KE, Habib FK. Oestrogen and benign prostatic hyperplasia: effects on stromal cell proliferation and local formation from androgen. J Endocrinol 2008; 197(3):483-91. doi: 10.1677/joe-07-0470 [Crossref] [ Google Scholar]
- Xu G, Dai G, Huang Z, Guan Q, Du C, Xu X. The etiology and pathogenesis of benign prostatic hyperplasia: the roles of sex hormones and anatomy. Res Rep Urol 2024; 16:205-14. doi: 10.2147/rru.S477396 [Crossref] [ Google Scholar]
- Naber KG, Weidner W. Chronic prostatitis-an infectious disease?. J Antimicrob Chemother 2000; 46(2):157-61. doi: 10.1093/jac/46.2.157 [Crossref] [ Google Scholar]
- Kim EH, Larson JA, Andriole GL. Management of benign prostatic hyperplasia. Annu Rev Med 2016; 67:137-51. doi: 10.1146/annurev-med-063014-123902 [Crossref] [ Google Scholar]
- Silva V, Grande AJ, Peccin MS. Physical activity for lower urinary tract symptoms secondary to benign prostatic obstruction. Cochrane Database Syst Rev 2019; 4(4):CD012044. doi: 10.1002/14651858.CD012044.pub2 [Crossref] [ Google Scholar]
- McConnell JD, Bruskewitz R, Walsh P, Andriole G, Lieber M, Holtgrewe HL. The effect of finasteride on the risk of acute urinary retention and the need for surgical treatment among men with benign prostatic hyperplasia Finasteride Long-Term Efficacy and Safety Study Group. N Engl J Med 1998; 338(9):557-63. doi: 10.1056/nejm199802263380901 [Crossref] [ Google Scholar]
- Thompson IM, Goodman PJ, Tangen CM, Lucia MS, Miller GJ, Ford LG. The influence of finasteride on the development of prostate cancer. N Engl J Med 2003; 349(3):215-24. doi: 10.1056/NEJMoa030660 [Crossref] [ Google Scholar]
- Andriole GL, Bostwick D, Brawley OW, Gomella L, Marberger M, Montorsi F. The effect of dutasteride on the usefulness of prostate specific antigen for the diagnosis of high grade and clinically relevant prostate cancer in men with a previous negative biopsy: results from the REDUCE study. J Urol 2011; 185(1):126-31. doi: 10.1016/j.juro.2010.09.011 [Crossref] [ Google Scholar]
- Corona G, Tirabassi G, Santi D, Maseroli E, Gacci M, Dicuio M. Sexual dysfunction in subjects treated with inhibitors of 5α-reductase for benign prostatic hyperplasia: a comprehensive review and meta-analysis. Andrology 2017; 5(4):671-8. doi: 10.1111/andr.12353 [Crossref] [ Google Scholar]
- Leliefeld HH, Debruyne FM, Reisman Y. The post-finasteride syndrome: possible etiological mechanisms and symptoms. Int J Impot Res 2025; 37(6):414-21. doi: 10.1038/s41443-023-00759-5 [Crossref] [ Google Scholar]
- Gacci M, Corona G, Vignozzi L, Salvi M, Serni S, De Nunzio C. Metabolic syndrome and benign prostatic enlargement: a systematic review and meta-analysis. BJU Int 2015; 115(1):24-31. doi: 10.1111/bju.12728 [Crossref] [ Google Scholar]
- Wilt TJ, Ishani A, Rutks I, MacDonald R. Phytotherapy for benign prostatic hyperplasia. Public Health Nutr 2000; 3(4a):459-72. doi: 10.1017/s1368980000000549 [Crossref] [ Google Scholar]
- Wilt T, Ishani A, Mac Donald R, Rutks I, Stark G. Pygeumafricanum for benign prostatic hyperplasia. Cochrane Database Syst Rev 2002; 1998(1):CD001044. doi: 10.1002/14651858.Cd001044 [Crossref] [ Google Scholar]
- Wilt T, Ishani A, MacDonald R, Stark G, Mulrow C, Lau J. Beta-sitosterols for benign prostatic hyperplasia. Cochrane Database Syst Rev 2000; 1999(2):CD001043. doi: 10.1002/14651858.Cd001043 [Crossref] [ Google Scholar]
- Fourcade RO, Théret N, Taïeb C. Profile and management of patients treated for the first time for lower urinary tract symptoms/benign prostatic hyperplasia in four European countries. BJU Int 2008; 101(9):1111-8. doi: 10.1111/j.1464-410X.2008.07498.x [Crossref] [ Google Scholar]
- Schubert SY, Lansky EP, Neeman I. Antioxidant and eicosanoid enzyme inhibition properties of pomegranate seed oil and fermented juice flavonoids. J Ethnopharmacol 1999; 66(1):11-7. doi: 10.1016/s0378-8741(98)00222-0 [Crossref] [ Google Scholar]
- Faria A, Calhau C. The bioactivity of pomegranate: impact on health and disease. Crit Rev Food Sci Nutr 2011; 51(7):626-34. doi: 10.1080/10408391003748100 [Crossref] [ Google Scholar]
- Consoli V, Burò I, Gulisano M, Castellano A, D’Amico AG, D’Agata V. Evaluation of the antioxidant and antiangiogenic activity of a pomegranate extract in BPH-1 prostate epithelial cells. Int J Mol Sci 2023; 24(13):10719. doi: 10.3390/ijms241310719 [Crossref] [ Google Scholar]
- Seeram NP, Adams LS, Henning SM, Niu Y, Zhang Y, Nair MG. In vitro antiproliferative, apoptotic and antioxidant activities of punicalagin, ellagic acid and a total pomegranate tannin extract are enhanced in combination with other polyphenols as found in pomegranate juice. J Nutr Biochem 2005; 16(6):360-7. doi: 10.1016/j.jnutbio.2005.01.006 [Crossref] [ Google Scholar]
- Jeune MA, Kumi-Diaka J, Brown J. Anticancer activities of pomegranate extracts and genistein in human breast cancer cells. J Med Food 2005; 8(4):469-75. doi: 10.1089/jmf.2005.8.469 [Crossref] [ Google Scholar]
- Pantuck AJ, Leppert JT, Zomorodian N, Aronson W, Hong J, Barnard RJ. Phase II study of pomegranate juice for men with rising prostate-specific antigen following surgery or radiation for prostate cancer. Clin Cancer Res 2006; 12(13):4018-26. doi: 10.1158/1078-0432.Ccr-05-2290 [Crossref] [ Google Scholar]
- Ammar AE, Esmat A, Hassona MD, Tadros MG, Abdel-Naim AB, Guns ES. The effect of pomegranate fruit extract on testosterone-induced BPH in rats. Prostate 2015; 75(7):679-92. doi: 10.1002/pros.22951 [Crossref] [ Google Scholar]
- Li Y, Guo C, Yang J, Wei J, Xu J, Cheng S. Evaluation of antioxidant properties of pomegranate peel extract in comparison with pomegranate pulp extract. Food Chem 2006; 96(2):254-60. doi: 10.1016/j.foodchem.2005.02.033 [Crossref] [ Google Scholar]
- Trevor AJ, Katzung BG, Kruidering-Hall MM, Masters SB. Drug evaluation & regulation. Katzung & trevor’s pharmacology: Examination & board review. 10th ed. New York: McGraw-Hill Companies; 2013.
- González-Sarrías A, García-Villalba R, Núñez-Sánchez MÁ, Tomé-Carneiro J, Zafrilla P, Mulero J. Identifying the limits for ellagic acid bioavailability: a crossover pharmacokinetic study in healthy volunteers after consumption of pomegranate extracts. J Funct Foods 2015; 19(Pt A):225-35. doi: 10.1016/j.jff.2015.09.019 [Crossref] [ Google Scholar]
- Whitehead AL, Julious SA, Cooper CL, Campbell MJ. Estimating the sample size for a pilot randomised trial to minimise the overall trial sample size for the external pilot and main trial for a continuous outcome variable. Stat Methods Med Res 2016; 25(3):1057-73. doi: 10.1177/0962280215588241 [Crossref] [ Google Scholar]
- Sreekumar A, Simmons MN, Lee TJ, Sharma A, Saini S. Therapeutic potential of pomegranate juice-derived nanovesicles in nude mouse benign prostatic hyperplasia (BPH) xenograft model. Sci Rep 2023; 13(1):12427. doi: 10.1038/s41598-023-39511-w [Crossref] [ Google Scholar]
- Nwachuku EO, Boisa N, Obisike UA. Pomegranate seed extract: a strong antioxidant against benign prostatic hyperplasia induced oxidative stress in albino Wistar rats. Journal of Cancer and Tumor International 2021; 11(4):50-60. doi: 10.9734/jcti/2021/v11i430160 [Crossref] [ Google Scholar]
- Nickel JC. Inflammation and benign prostatic hyperplasia. Urol Clin North Am 2008; 35(1):109-15; vii. doi: 10.1016/j.ucl.2007.09.012 [Crossref] [ Google Scholar]
- Kessler OJ, Keisari Y, Servadio C, Abramovici A. Role of chronic inflammation in the promotion of prostatic hyperplasia in rats. J Urol 1998; 159(3):1049-53. [ Google Scholar]
- Di Silverio F, Gentile V, De Matteis A, Mariotti G, Giuseppe V, Luigi PA. Distribution of inflammation, pre-malignant lesions, incidental carcinoma in histologically confirmed benign prostatic hyperplasia: a retrospective analysis. Eur Urol 2003; 43(2):164-75. doi: 10.1016/s0302-2838(02)00548-1 [Crossref] [ Google Scholar]
- Mishra VC, Allen DJ, Nicolaou C, Sharif H, Hudd C, Karim OM. Does intraprostatic inflammation have a role in the pathogenesis and progression of benign prostatic hyperplasia?. BJU Int 2007; 100(2):327-31. doi: 10.1111/j.1464-410X.2007.06910.x [Crossref] [ Google Scholar]
- Nickel JC, Roehrborn CG, O’Leary MP, Bostwick DG, Somerville MC, Rittmaster RS. The relationship between prostate inflammation and lower urinary tract symptoms: examination of baseline data from the REDUCE trial. Eur Urol 2008; 54(6):1379-84. doi: 10.1016/j.eururo.2007.11.026 [Crossref] [ Google Scholar]
- Roehrborn CG. Definition of at-risk patients: baseline variables. BJU Int 2006; 97 Suppl 2:7-11. doi: 10.1111/j.1464-410X.2006.06098.x [Crossref] [ Google Scholar]
- Rettig MB, Heber D, An J, Seeram NP, Rao JY, Liu H. Pomegranate extract inhibits androgen-independent prostate cancer growth through a nuclear factor-kappaB-dependent mechanism. Mol Cancer Ther 2008; 7(9):2662-71. doi: 10.1158/1535-7163.Mct-08-0136 [Crossref] [ Google Scholar]
- Thomas R, Williams M, Sharma H, Chaudry A, Bellamy P. A double-blind, placebo-controlled randomised trial evaluating the effect of a polyphenol-rich whole food supplement on PSA progression in men with prostate cancer--the UK NCRN Pomi-T study. Prostate Cancer Prostatic Dis 2014; 17(2):180-6. doi: 10.1038/pcan.2014.6 [Crossref] [ Google Scholar]
- Paller CJ, Ye X, Wozniak PJ, Gillespie BK, Sieber PR, Greengold RH. A randomized phase II study of pomegranate extract for men with rising PSA following initial therapy for localized prostate cancer. Prostate Cancer Prostatic Dis 2013; 16(1):50-5. doi: 10.1038/pcan.2012.20 [Crossref] [ Google Scholar]
- Obisike UA, Nwachuku EO, Boisa N. Anti-tumour potential of Punica granatum (pomegranate) seed in testosterone-induced benign prostate hyperplastic Wistar albino rats. Asian J Res Rep Urol 2021; 4(4):143-56. [ Google Scholar]
- Adhami VM, Siddiqui IA, Syed DN, Lall RK, Mukhtar H. Oral infusion of pomegranate fruit extract inhibits prostate carcinogenesis in the TRAMP model. Carcinogenesis 2012; 33(3):644-51. doi: 10.1093/carcin/bgr308 [Crossref] [ Google Scholar]
- Hikal WM, Said-Al Ahl HA, Tkachenko KG, Mahmoud AA, Bratovcic A, Hodžić S. An overview of pomegranate peel: a waste treasure for antiviral activity. Trop J Nat Prod Res 2022; 6(1):15-9. doi: 10.26538/tjnpr/v6i1.3 [Crossref] [ Google Scholar]
- Khwairakpam AD, Bordoloi D, Thakur KK, Monisha J, Arfuso F, Sethi G. Possible use of Punica granatum (pomegranate) in cancer therapy. Pharmacol Res 2018; 133:53-64. doi: 10.1016/j.phrs.2018.04.021 [Crossref] [ Google Scholar]
- Cheshomi H, Bahrami AR, Rafatpanah H, Matin MM. The effects of ellagic acid and other pomegranate (Punica granatum L) derivatives on human gastric cancer AGS cells. Hum Exp Toxicol 2022; 41:9603271211064534. doi: 10.1177/09603271211064534 [Crossref] [ Google Scholar]