Pharmaceutical Sciences. 31(4):357-378.
doi: 10.34172/PS.025.42290
Research Article
Efficacy and Safety of SGLT2 Inhibitors in Individuals with Sold Organ Transplantation: A Systematic Review and Meta-analysis
Sajad Khiali Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Validation, Writing – original draft, Writing – review & editing, 1, 2 
Mohammadreza Ardalan Conceptualization, Methodology, Project administration, Writing – review & editing, 3
Ali Sharifi Validation, 4
Amin Sadrazar Methodology, 5
Afra Rezagholizadeh Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Writing – original draft, Writing – review & editing, 6
Parvin Sarbakhsh Formal analysis, Software, 7
Zeinab Javadivala Formal analysis, Software, 8
Sama Samankan Data curation, Resources, 6
Amin Aghabalzadeh Data curation, Investigation, Resources, 6
Mohammad Reza Afshar Mogaddam Project administration, 2
Afshin Gharekhani Conceptualization, Data curation, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing, 2, *
Mahboob Nemati Project administration, Supervision, Validation, 2, 9, *
Author information:
1Cardiovascular Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
2Food and Drug Safety Research Center, Pharmaceutical Sciences Institute, Tabriz University of Medical Sciences, Tabriz, Iran
3Chronic Kidney Disease Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
4Department of General Surgery, Imam Reza Hospital, Tabriz University of Medical Sciences, Tabriz, Iran
5Liver and Gastrointestinal Diseases Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
6Department of Clinical Pharmacy, Faculty of Pharmacy, Tabriz University of Medical Sciences, Tabriz, Iran
7Department of Statistics and Epidemiology, Faculty of Public Health, Tabriz University of Medical Sciences, Tabriz, Iran
8Department of Health Education & Promotion, Faculty of Health, Tabriz University of Medical Sciences, Tabriz, Iran
9Pharmaceutical Analysis Research Center, Pharmaceutical Sciences Institute, Tabriz University of Medical Sciences, Tabriz, Iran
Abstract
Despite the growing body of evidence supporting the beneficial effects of sodium-glucose transporter 2 (SGLT-2) inhibitors on metabolic, cardiovascular, renal, and mortality outcomes in the wide range of diseases, clinical data in patients with solid organ transplantation (SOT) is limited. A systematic literature search was conducted in PubMed, Scopus, and Web of Science from database inception until April 14, 2025, to evaluate the efficacy and safety of SGLT-2 inhibitors in patients with SOT. Among 25 studies, 18 included kidney transplant recipients. There was considerable heterogeneity between the remaining studies regarding design, setting, and outcomes. The meta-analysis of two interventional studies showed the beneficial effects of SGLT-2 inhibitors on body mass index (BMI) (-2.564, 95% CI: -4.982 to -0.146, I2=0%, P=0.0377), weight (-0.800, 95% CI: -0.878 to -0.722, I2=0%, P<0.0001), and hemoglobin A1c (HbA1c) (-0.447, 95% CI: 0.085 to 0.810, I2=0%, P=0.0155) in the kidney transplant population. The mortality benefits of SGLT-2 inhibitors in the kidney transplant population have been shown in observational studies with large sample sizes. Despite the benefits of SGLT-2 inhibitors on metabolic outcomes and their satisfactory safety profiles represented in most eligible studies, these medications should be used with caution in patients with SOT, particularly in high-risk patients. Additional well-designed studies are needed to reveal the efficacy and safety of SGLT-2 inhibitors in patients with SOT.
Keywords: SGLT-2 inhibitors, Transplantation, Solid organ transplant
Copyright and License Information
© 2025 The Author(s).
This is an open access article and applies the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Introduction
Solid organ transplantation (SOT) has considerably evolved in the recent several years, transforming from an experimental procedure into a standard of care. Based on the United Network for Organ Sharing (UNOS) database for solid-organ transplants, more than 2 million life-years have been saved by SOTs during a 25-year study period.1 However, despite advancements in graft performance and patient survival, individuals with SOT continue to face neurological, gastrointestinal, cardiovascular, infectious, malignant, renal, metabolic, and endocrine complications after transplantation.2
Sodium-glucose transporter 2 (SGLT2) inhibitors have gained considerable attention due to their wide range of medical benefits beyond controlling blood glucose levels.3 Over the past decade, large and well-designed clinical trials have demonstrated noteworthy promising effects of SGLT-2 inhibitors in multiple therapeutic targets, thereby altering the treatment paradigm for diabetes mellitus (DM), chronic kidney disease (CKD), and heart failure (HF).4,5 Further studies have also revealed their beneficial effects in conditions such as ischemic heart diseases, arrhythmia, fatty liver disease, and kidney stones.6-8
Based on the literature, SGLT-2 inhibitors may be beneficial for patients who have undergone SOT; however, well-designed studies and robust data regarding their use in these patients are still lacking.9 From a pharmacological perspective, SGLT-2 inhibitors can provide beneficial effects for individuals with SOT through different mechanisms. For example, SGLT-2 inhibitors could reduce weight and improve glycemic control, which is linked to a decreased risk of transplant complications, such as new-onset diabetes after transplantation (NODAT), a post-transplant metabolic complication that develops among kidney allograft recipients, with about 4%-27% incidence rate, leading to improved clinical outcomes.10 Besides, proteinuria is common among organ transplant patients and poses a major risk for organ failure, cardiovascular disease, and overall mortality. It has been shown that SGLT-2 inhibitors could improve post-transplant proteinuria by lowering intraglomerular pressure, blood pressure, and hyperfiltration.11
Although SGLT-2 inhibitors have been shown to generally be well-tolerated, clinical trial data from non-transplant populations has proposed that SGLT-2 inhibitors could increase the risk of vaginal yeast and urinary tract infections (UTIs), as well as serious adverse drug reactions (ADRs) such as dehydration, acute kidney injury (AKI), and diabetic ketoacidosis.12 Notably, individuals with SOT are at higher risk for ADRs due to factors such as impaired renal function, the use of immunosuppressive medications, and immunodeficiency.13 While several studies have assessed the safety of SGLT-2 inhibitors in this population, robust clinical data is still lacking.14
Considering the above, we conducted an updated systematic review and meta-analysis to evaluate the efficacy and safety of SGLT-2 inhibitors in individuals with SOT.
Methods
Study design
The present study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for reporting systematic reviews. The protocol of this systematic review and meta-analysis has been registered in the International Prospective Register of Systematic Reviews (PROSPERO) database with the registration number CRD42024575119.
Search strategy
We conducted a systematic review by searching the MEDLINE (PubMed), Scopus (Elsevier), and Web of Science (Clarivate Analytics) databases from their inception until April 14, 2025, to gather relevant studies. The additional studies were extracted using Google Scholar, the World Health Organization (WHO), and the United States (US) Food and Drug Administration (FDA) websites. Additionally, the references of the included studies and the most related reviews were checked manually.
Two authors (S.K. and A.R.) independently performed the literature search, publication screening, and eligibility assessment. Any disagreement between the two was resolved by discussion and/or involving the third review author (A.G.). We applied the Population, Intervention, Comparison, and Outcome (PICO) framework to plan the concept map and to define the inclusion and exclusion criteria.15 Additionally, the MeSH search of PubMed was used to select the most applicable keywords.
Inclusion criteria
The inclusion criteria of this systematic review were as follows: the setting of the non-randomized studies of interventions (NRSIs) or randomized clinical trials (RCTs); population/test sample of individuals with SOT; intervention of SGLT2 inhibitor administration; comparison of placebo, standard care, or none, and outcomes/objectives of safety or efficacy.
Exclusion criteria
In silico, in vitro, and animal experiments; case reports; clinical trial protocols; practice guidelines; any type of review; book chapters; editorial or commentary publications; duplicate articles; publications written in any language other than English; and studies using only a single dose of SGLT2 inhibitors were excluded from the systematic review.
Search terms
Our search terms were as follows: (“sodium-glucose transporter 2 inhibitor” OR “empagliflozin” OR “canagliflozin” OR “dapagliflozin” OR “ertugliflozin OR “ipragliflozin” OR “licogliflozin” OR “remogliflozin” OR “sergliflozin” OR “bexagliflozin” OR “sotagliflozin” OR “luseogliflozin” OR “tofogliflozin” OR “henagliflozin” OR “velagliflozin” OR “janagliflozin” OR “mizagliflozin” OR “enavogliflozin” OR “rongliflozin” OR “tianagliflozin”) AND (“graft” OR “transplant” OR “allograft” OR “allotransplant” OR “Homograft”). The detailed search strategies used in each database are shown in Table S1 (See Supplementary file 1).
Data extraction
To ensure the accuracy and consistency of data extraction from selected publications, we utilized a checklist adapted from the Cochrane Collaboration data collection form. This checklist comprised five key sections: General Information, Methods, Participants, Intervention Group, and Outcomes.
The General Information section included details on study identification, first author, publication year, and reference citation. The Methods section covered the study’s aim, design, and duration. The Participants section outlined population description, setting, inclusion and exclusion criteria, and relevant sociodemographic characteristics. The Intervention Group section detailed the number of participants, description of the intervention, including type of medication and daily dose, treatment duration, administration details, medical providers, and economic information. Lastly, the Outcomes section specified the outcome measure, time points, validity, assumed risk estimate, and power.
Risk of bias assessment in included studies
To assess the potential for systematic errors in observational studies we used the Risk of Bias in Non-randomized Studies of Exposures (ROBINS-E) tool,16 which includes bias due to: (a) confounding; (b) exposure misclassification; (c) selection of participants into the study; (d) missing data; (e) outcome measurement error; and (f) selective reporting of results. For each domain, we scored the risk of bias as low, some concern, high, or no information. Any disagreement was resolved by discussion and consensus by the two scorers (Z.J. and S.K.).
To assess the risk of bias (ROB) in RCTs we applied Cochrane’s RoB 2 tool which has five domains, including the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result.17 The visualization of the risk of bias assessment results was done using the online robvis tool.18
Due to the low estimation power of publication bias tools in meta-analyses of ten or fewer studies and the high confounding risk of the NRSIs, the publication bias tests were not operated.19,20
Statistical data analysis
The meta-analysis was conducted using a random-effects model to assess the pooled effect sizes across two studies with different designs; including a one-group pre-post interventional study and a two-group pre-post interventional study with an intervention group and a control group. Due to the differences in study designs, the control group data from the two-group study were excluded. The analysis was performed by pooling the pre-post data from the intervention group of the two-group study with the pre-post data from the one-group study. Where required, transformations were applied to approximate mean and standard deviation (SD) from the median and interquartile range (IQR). Statistical heterogeneity between studies was assessed using I2 statistics. A rough guide for interpreting the I2 index based on the Cochrane Handbook for systematic reviews of interventions is as follows: 0% to 40%: not important, 30% to 60%: moderate, 50% to 90%: substantial, and 75% to 100%: considerable heterogeneity.21 All analyses were conducted in Stata Version 17 (STATA Corporation, College Station, Texas, USA). Results were reported as mean differences (MDs) with 95% confidence intervals (CIs). A P value < 0.05 was considered statistically significant. Forest plots were generated to visualize the findings.
Results
Study selection process
A total of 1618 studies were primarily obtained from searching the literature. Following duplicate removal and screening of the records by their titles and abstracts, 1116 studies were entered into the eligibility assessment. A total of 884 studies were excluded by reviewing the titles and abstracts. Then, by reading the full text, 207 records were excluded with reasons, including irrelevant/on other drugs studies (n = 77), review/systematic reviews and meta-analyses (n = 47), case reports (n = 22) in-vitro/in-silico/animal experiments (n = 20), editorials/commentaries (n = 18), letters (n = 13), non-English papers (n = 6), or duplicates (n = 4). Finally, 25 studies were entered into the systematic review. The PRISMA flow diagram is shown in Figure 1.
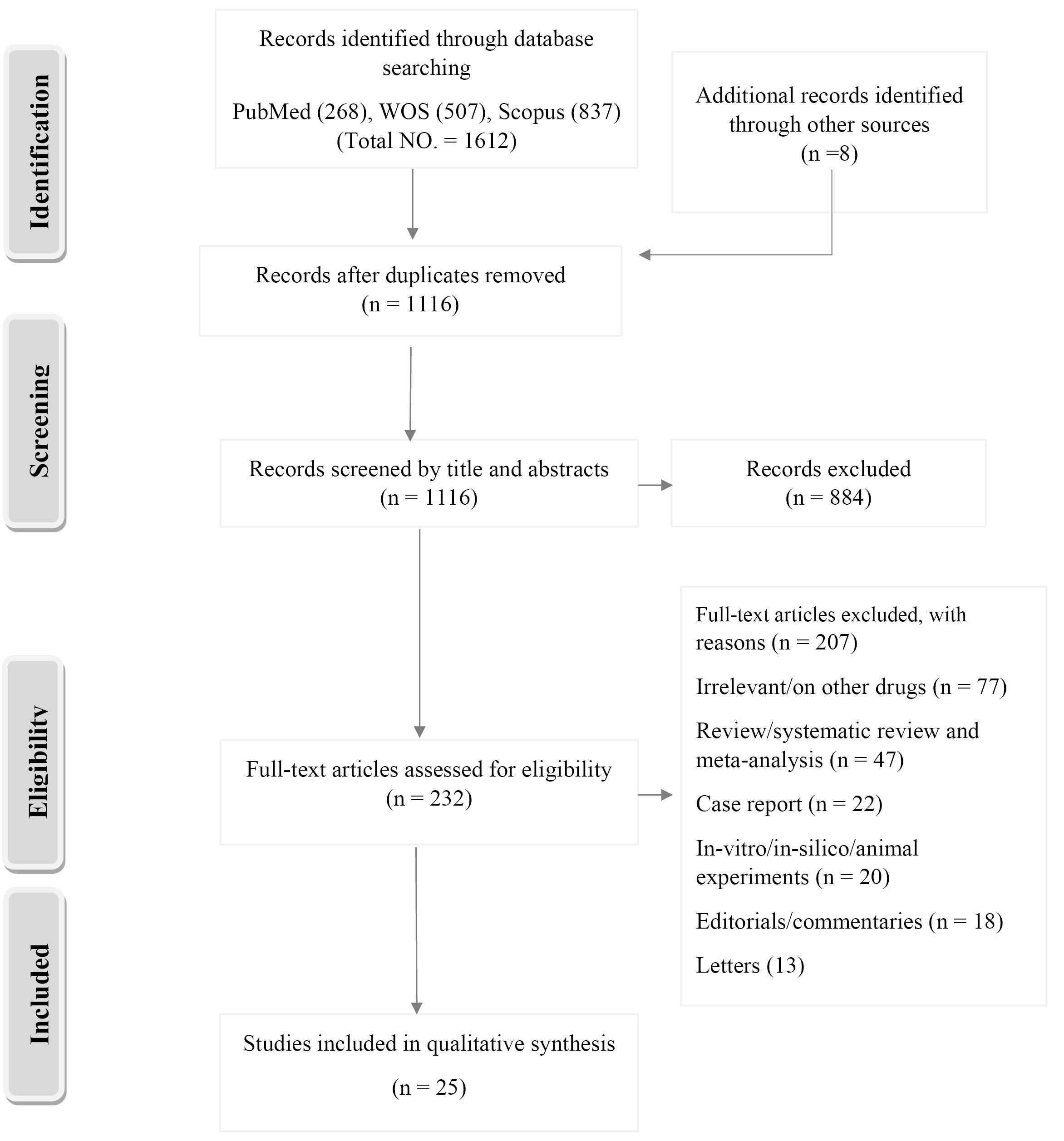
Figure 1.
Study selection flow diagram. Preferred reporting items for systematic reviews and meta-analyses (PRISMA)
.
Study selection flow diagram. Preferred reporting items for systematic reviews and meta-analyses (PRISMA)
Assessment of risk of bias
Among non-randomized studies of exposure, five out of the 10 out of 19 had an overall high risk of bias. In most cases, this was due to a lack of control for potential confounding variables or bias due to departures from intended exposures and missing data. Seven studies were classified as having some concern because there was no adjustment for known confounding factors and discontinued intervention during the follow-up (Figure 2A and 2B). Among two interventional studies, one had a high risk of bias due to a lack of randomization, the other had a low risk of bias (Figure 3A and 3B).
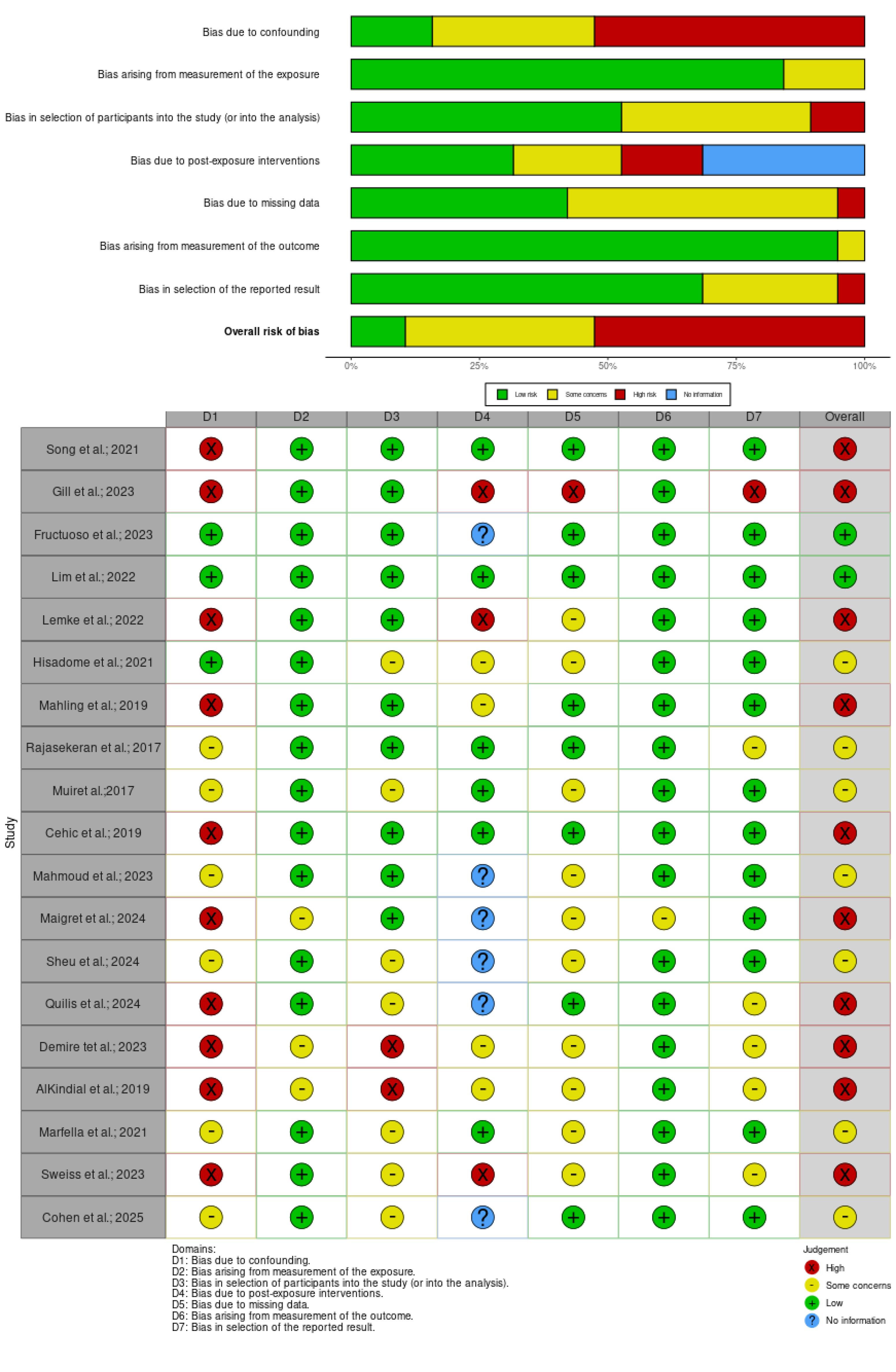
Figure 2.
Risk of bias assessment results for non-randomized studies according to the ROBINS-E tool. (A) Traffic light plot of the domain-level judgments for each result (B) Weighted bar plot of the distribution of risk-of-bias judgments within each bias domain
.
Risk of bias assessment results for non-randomized studies according to the ROBINS-E tool. (A) Traffic light plot of the domain-level judgments for each result (B) Weighted bar plot of the distribution of risk-of-bias judgments within each bias domain
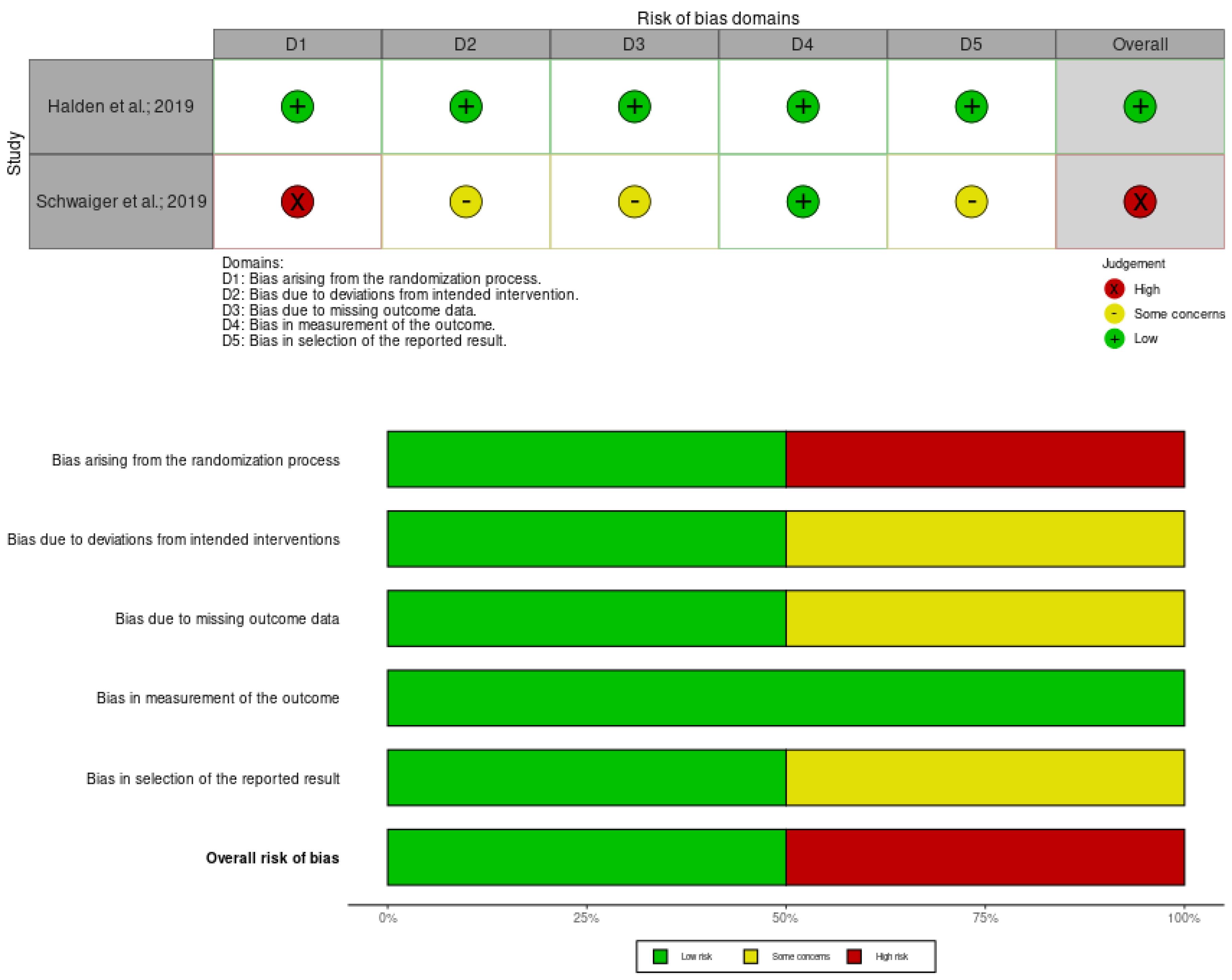
Figure 3.
Risk of bias assessment results for randomized controlled trials according to the RoB2 tool. (A) Traffic light plot of the domain-level judgments for each result (B) Weighted bar plot of the distribution of risk-of-bias judgments within each bias domain
.
Risk of bias assessment results for randomized controlled trials according to the RoB2 tool. (A) Traffic light plot of the domain-level judgments for each result (B) Weighted bar plot of the distribution of risk-of-bias judgments within each bias domain
Study characteristics
A total of 8138 individuals from 25 studies, including 19 observational studies, 4 case series, and 2 RCTs were included in the systematic review. The studies were performed in the U.S. (n = 3), Canada (n = 2), Japan (n = 2), Australia (n = 2), Spain (n = 2), United Arabic Emirates (n = 2), France (n = 1) Germany (n = 1), Austria (n = 1), Norway (n = 1), Italy (n = 1), Korea (n = 1), Turkey (n = 1) Kuwait (n = 1), Qatar (n = 1), India (n = 1), Israel (1), and Taiwan (n = 1). The majority of studies were carried out among kidney transplant patients, followed by heart, simultaneous pancreas/kidney, and liver transplant patients. Notably, one observational study and one case series included only non-diabetic patients, while 18 remaining did not exclude patients with NODAT or pre-exciting DM. Different doses and durations of SGLT-2 inhibitors, including empagliflozin, canagliflozin, dapagliflozin, ipragliflozin, luseogliflozin, and ertugliflozin have been used. As shown in Table 1, there was considerable heterogeneity between the studies regarding the time to SGLT-2 inhibitors initiation, treatment period, and follow-up duration. The most common concomitant medications were calcineurin inhibitor, mammalian target of rapamycin (mTOR) inhibitors, mycophenolate, oral anti-diabetic agents hydroxymethylglutaryl-coenzyme A (HMG-CoA) reductase inhibitors, and insulin. The detailed characteristics and outputs of the included studies in the systematic review are presented in Tables 1 and 2, respectively.
Table 1.
Characteristics of the included studies
|
Authors; Year; Location
|
Setting
|
Sample size (SGLT-2 inhibitor %)
|
Sex; Age (Years)
|
Transplant type
|
Kidney function status
|
Diabetes status
|
SGLT-2 inhibitor; dose
|
Other treatments
|
SGLT-2 inhibitors' initiation time after transplant
|
Follow-up period
|
| Halden et al22; 2019; Norway |
Single-center, double-blind, placebo-controlled clinical trial |
44 (50) |
Intervention:
F (29.4%);
Median (range): 63 (31-72)
Control: F (29.4%); 59 (21-75) |
Stable kidney transplant |
Less than 20% deviation in SrCr within the last two months |
NODAT with persistent hyperglycemia for at least one year after transplantation |
Empagliflozin; 10 mg/day |
CIs, everolimus, prednisolone, MMF, insulin, oral anti-diabetics, statin, anti-hypertensives, anti-platelets, and anticoagulants |
Over one year |
24 weeks |
| Schwaiger et al23; 2019; Austria |
Prospective, interventional, non-inferiority pilot study |
14 (100) |
F (50%); Mean (SD):
56.5 (7.9) |
Stable kidney transplant ( ≥ 6 months) |
eGFR ≥ 30 mL/min/1.73 m2 |
NODAT treated for ≥ 6 months on insulin therapy |
Empagliflozin; 10 mg/day |
CIs, MMF, glucocorticoids, insulin, anti-diabetics |
Mean (SD): 69.4 months (57.2) |
12 months |
| Song et al32; 2021; USA |
Single-center, retrospective, observational study |
50 (100) |
F (34%);
Mean (SD): 57.03 (13.14) |
Kidney transplant |
eGFR ≥ 30 mL/min/1.73 m2 |
Pre-existing T2DM or NODAT |
Empagliflozin (86%), canagliflozin (12%), dapagliflozin (2%); NR |
Tacrolimus, MMF, prednisolone, insulin, oral anti-diabetics |
Median (IQR): 319 days (112-696) |
6 months |
| Lim et al26; 2022; Korea |
Multi-center, retrospective cohort study |
2083 (11) |
F (32.8%);
Mean (SD): 52.4 (10.7) |
Kidney transplant |
Mean eGFR (SD): 68.2 (19.9) mL/min/1.73 m2 |
Pre-existing T2DM (77.2%) or NODAT (28.8%) |
Empagliflozin (66.4%), dapagliflozin (33.6%); NR |
CIs, corticosteroids, insulin, oral anti-diabetics |
NR |
Mean (SD):
9 (42.2) months |
| Fructuoso et al30; 2023; Spain |
Multi-center, retrospective cohort study |
339 (100) |
F (26.3%); Mean (SD):
61.6 (9.9) |
Kidney transplant |
Mean eGFR: 58.4 mL/min/1.73 m2 |
Pre-existing T2DM (39.5%) or NODAT (60.5%) |
Empagliflozin (56.9%), dapagliflozin (23.9%), canagliflozin (18.9%); NR |
CIs, MMF, mTOR inhibitors, prednisolone, insulin, oral anti-diabetics |
NR |
6-12 months |
| Maigret et al28; 2024; France |
Multi-center, prospective real-life study |
347 (100) |
F (23.6 %);
Median (IQR): 62.6 (52.1–69.5) |
Kidney transplant |
30 < eGFR < 60 mL/min/1.73 m2 (75.8%) |
DM (65.1%) |
Dapagliflozin (97%)
Empagliflozin (3%) |
Immunosuppression regimen, ACEi or ARB, anti-diabetics |
One year (87%)
Median (IQR): 6.7 years (2.8–13.5) |
Median (IQR): 12.0 (0.1–44.8) months |
| Hisadome et al25; 2021; Japan |
Retrospective, observational, single-center, IPTW analysis study |
85 (33) |
Intervention:
F (27.6%); Mean (SD): 56.4 (8.7)
Control:
F (27.6); 55.9 (10.2) |
Kidney transplant |
Intervention eGFR:
Mean (SD): 53.3 (17.1) mL/min/1.73 m2
Control:
46.2 (14.0) |
T2DM |
Canagliflozin (31.03), ipragliflozin (24.13), luseogliflozin (17.24%), empagliflozin (13.79%), dapagliflozin (10.34%) |
CIs, MMF or everolimus, methylprednisolone |
NR |
12 months |
| Sheu et al31; 2025; Taiwan |
Historical cohort from the TriNetX database |
3940 (50) |
Intervention:
F (36.8%); Mean (SD): 59.5 (11.3)
Control:
F (41.4%); 59.6 (11.5) |
Kidney transplant |
Intervention eGFR:
Mean (SD): 54 (22.5) mL/min/1.73 m2
Control:
53.5 (24.9) |
DM (100%) |
Dapagliflozin; 5-10 mg/day
Canagliflozin; 100–300 mg/day
Empagliflozin; 10 -25 mg/day
Ertugliflozin 5 -15 mg/day |
Immunosuppression regimen, ACEi or ARB, anti-diabetics |
Within 3 months |
Median: 3.4 years |
| Gill et al24; 2023; Canada |
Retrospective study (electronic outpatient transplant database) |
42 (100) |
F (24%); Mean (SD):
59 (12.3) |
Kidney transplant |
Mean eGFR: 71 mL/min/1.73 m2 |
DM (62%) |
Empagliflozin (88%), canagliflozin (10%), dapagliflozin (2%); NR |
Immunosuppression regimen, ACEi or ARB, diuretics, |
Mean:7 years |
3 months |
| Mahling et al27; 2019; Germany |
Prospective observational study |
10 (100) |
F (20%);
Median (IQR):
66 (56-73) |
Kidney transplant |
Median eGFR: 57 (range: 47–73) mL/min/1.73 m2 |
NODAT (40%), T2DM (60%) |
Empagliflozin; NR |
CIs, MMF, corticosteroids, insulin, anti- diabetics |
Median (IQR): 5.9 (4.4–8.8) years |
Median (IQR): 12 (5.3–12.0) months |
| Quilis et al29; 2025; Spain |
Observational study |
22 (100) |
F (31.8%); Median: 58 |
Kidney transplant |
Median eGFR: 31 (range: 23.7 – 45.2) mL/min/1.73 m2 |
Non-diabetic |
Dapagliflozin (91%) |
Immunosuppression regimen, ACEi or ARB |
Median: 67 months |
6 months |
| Demir et al9; 2023; Turkey |
Retrospective cohort study |
57 (63) |
F (36.8%);
Mean (SD): 51.30 (10.98) |
Kidney transplant |
No SGLT-2 inhibitor eGFR:
Mean (SD): 73.20 (19.72)
SGLT-2 inhibitor: 71.94 (18.17) mL/min/1.73 m2 |
T2DM (45.6%), NODAT (54.4%) |
Empagliflozin (NR), dapagliflozin (NR); NR |
Immunosuppression regimen, anti-diabetics |
Within 3 months (N = 11); after 3 months (N = 25) |
12 months |
| Cohen et al33; 2025; Israel |
Retrospective cohort study |
480 (50%) |
F (20%); SGLT-2 inhibitor:
Median: 63
Control: 64 |
Kidney transplant |
eGFR > 30 mL/min/1.73 m2 |
SGLT-2 inhibitor: T2DM (57%), NODAT (43%)
Control:
T2DM (54 %), NODAT (46%) |
Empagliflozin (NR), dapagliflozin (NR); NR |
Immunosuppression regimen, anti-hypertensive medications, anti-diabetics |
NR |
3 years |
| Shah et al38; 2019; India |
Prospective case series |
25 (100) |
F (4%); Mean (SD): 53.8 (7.1) |
Stable kidney transplant |
eGFR > 60 mL/min/1.73 m2 |
Pre-existing T2DM (80%) or NODAT (20%) |
Canagliflozin; 100 mg /day |
Tacrolimus, MMF or azathioprine, prednisolone, antihypertensives, lipid-lowering agent, oral anti-diabetics |
Mean: 2.7 years (0.2 to 13.2) |
At least 6 months |
| Miyazaki et al37; 2022; Japan |
Case series |
5 (100) |
F(0%); Mean (SD): 58.4 (5.6) |
Kidney transplant with metabolic syndrome |
Chronic kidney disease G3a-4 |
Non-diabetic |
Empagliflozin; 10 mg/day |
CIs, MMF, everolimus, glucocorticoids |
Range: 4.3-24 years |
8 to 24 months |
| Attallah et al35; 2019; UAE |
Case series |
8 (100) |
F (50%); Mean (SD): 45.87 (6.64) |
Kidney transplant |
Average creatinine: 88.5 mmol/L |
NODAT (50%); pre-existing DM (50%) |
Empagliflozin; 25 mg/day |
Tacrolimus, MMF, prednisolone |
Mean: 21 months |
12 months |
| Gul et al36; 2021; Qatar |
Case series |
4 (100) |
F (25%); Mean (SD): 56.75 (6.21) |
Kidney transplant |
NR |
NODAT (75%), T2DM (25%) |
Empagliflozin; 10 mg/day |
Antidiabetics, Immunosuppression regimen |
5 to 13 years |
NR |
| AlKindi et al34; 2019; UAE |
Observational |
8 (100) |
F (25%);
Mean (SD): 56.8 (13.70) |
Kidney transplant |
Mean eGFR (SD): 75.75 (13.38) mL/min/1.73 m2 |
NODAT (75%), T2DM (25%) |
Empagliflozin (75%) dapagliflozin (25%); NR |
Antidiabetics, Immunosuppression regimen |
9.6 years |
12 months |
| Sweiss et al42; 2023; USA |
Single-enterer retrospective program evaluation study |
49 (100) |
F (29%); Median (IRQ): 63 (58-68.5) |
Liver (53%), kidney (37%), lung (8%), liver-kidney (2%) |
Median eGFR (IQR): 66 (54-85) |
DM |
Empagliflozin (65%), dapagliflozin (27%), canagliflozin (8%); NR |
Immunosuppressant agents, antihypertensives, anti-diabetics |
Median (IQR): 39 (16-73) months |
At least 12 months |
| Rajasekeran et al44; 2017; Canada |
Retrospective observational cohort |
10 (100) |
SPKT:
F (50%); Mean (SD): 49.4 (8.9)
Kidney:
F (17%); 61.6 (12.6) |
SPKT (N = 4), kidney (6) |
SPKT eGFR:
Mean (SD): 60 (14) mL/min/1.73 m2
Kidney eGFR:
78 (18.2) |
NODAT (80%); DM (20%) |
Canagliflozin; NR |
Immunosuppressant agents, antihypertensives, anti-diabetics |
SPKT:
Mean (SD): 3.5 (3.9) years for 5.6 (3.4)
Kidney:
4.4 (3.3) for 10. (4.2) |
80.5 person-months |
| Lemke et al45; 2022; USA |
Retrospective, descriptive study (electronic medical records) |
39 (100) |
F (26%);
Median (IQR) 57 (48–66) |
Kidney transplant (98%), SPKT (2%); liver and kidney (2%) |
NR |
Pre-existing T2DM (56%), NODAT (44%) |
Dapagliflozin, (61%), canagliflozin (31%), empagliflozin (8%) |
CIs, MMF, azathioprine, belatacept, prednisone, insulin, oral anti-diabetics |
Median (IQR): 28 (16–60) months |
NR |
| Muir et al41; 2017; Australia |
Single-center, retrospective observational study |
90 (18) |
F (29%);
Mean (SD): 55.8 (14.4) |
Heart transplant |
Empagliflozin eGFR:
Mean (SD): 57 (18) mL/min/1.73 m2
Without empagliflozin eGFR:
54 (20) |
NODAT or pre-existing T2DM |
Empagliflozin;10 mg (52.6%) or 25 mg (47.4%) |
CIs, prednisolone, everolimus, insulin, oral anti-diabetics, furosemide |
Median (IQR): 5.5 years (0-11) |
At least 3 months |
| Cehic et al40; 2019; Australia |
Single-center, retrospective observational study |
101 (22) |
Intervention:
F (23%); Mean (SD): 59.3 (11.9)
Control:
F (32%); 58.0 (11.4) |
Heart transplant |
Intervention eGFR:
Median (IQR): 48 (43–61) mL/min/1.73 m2
Control eGFR:
54 (41-74) |
NODAT or pre-existing T2DM |
Empagliflozin; 10 mg (45.45%), 25 mg (54.55%) |
CIs, prednisolone, everolimus, insulin, oral anti-diabetics, furosemide |
Median (IQR): 5.0 years (2.0-12.3) |
At least 12 months |
| Marfella et al39; 2021; Italy |
Prospective observational study |
77 (17) |
F (23.4%);
Non-diabetic:
Mean (SD): 50.9 (6.0)
Diabetic,no-SGLT-2 inhibitor: 52.7 (5.5)
Diabetic, SGLT-2 inhibitor: 51.3 (6.0) |
Heart transplant |
SrCr:
Non-diabetic:
Mean (SD): 1.0 (0.26)
Diabetic, No-SGLT-2 inhibitor: 1.1 (0.16)
Diabetic, SGLT-2 inhibitor: 1.1 (0.24) |
Non-diabetic (52%), T2DM (48%) |
Empagliflozin (58.8%), dapagliflozin (29.4%), canagliflozin (11.8%); NR |
CIs, prednisolone, everolimus, insulin, oral anti-diabetics |
At least 6 months before transplant |
12 months |
| Mahmoud et al43; 2023; Kuwait |
Single-center, retrospective observational study |
209 (47) |
F (40.5%); Median (IQR): 63 (56-68) |
Liver transplant |
Intervention eGFR:
Median: 67.2 mL/min/1.73 m2
Control eGFR: 63.8 |
T2DM (61.22%), NODAT (38.77%) |
Canagliflozin; 100–300 mg/day |
Thymoglobulin, basiliximab, CIs, Insulin, oral anti-diabetics, |
Mean: 84.2 |
12 months |
ACEi, Angiotensin-Converting Enzyme inhibitor; ARB, Angiotensin Receptor Blocker; CIs, Cornerstone Immunosuppressive Agents (Tacrolimus and Cyclosporine); DM, Diabetes Mellitus; eGFR, estimated Glomerular Filtration Rate; F, Female; GLP-1RAs, glucagon-like peptide-1 receptor agonists; IPTW, Inverse Probability of Treatment Weighting; IQR, Interquartile Range; MMF, Mycophenolate Mofetil; mTOR: mammalian Target of Rapamycin; NODAT, New Onset Diabetes After Transplant; NR, Not Reported; SD, Standard Deviation; SGLT-2, Sodium-Glucose Transporter 2; SPKT, Simultaneous Pancreas-Kidney Transplant; SrCr, Serum Creatinine; T2DM, Type 2 Diabetes Mellitus
Table 2.
Outcomes of the included studies
|
Study
|
Efficacy outcomes
|
Safety outcomes
|
| Halden et al22 |
Significant effects: intervention vs. control median (IQR); P-value
Weight (kg): -2.5 (-4.0, -0.05) vs. 1.0 (0.0, 2.0); P = 0.014
BMI (kg/m2): -0.80 (-1.4, 0.0) vs. 0.35 (0.0, 0.60); P = 0.011
HbA1c (%): -0.2 (-0.6, -0.1) vs. 0.1 (-0.1, 0.4); P = 0.025
Uric acid (µmol/L): -53 (-90, -38) vs. 0 (-15, 36); P < 0.001
Magnesium (mmol/L): 0.04 (0.00, 0.07) vs. 0.00 (-0.05, 0.02); P < 0.01
Hemoglobin (g/dL): 0.45 (-0.03, 0.83) vs. 0.0 (-0.40, 0.20); P = 0.047
Hematocrit: 0.01 (0.00, 0.02) vs. -0.01 (-0.01, 0.00); P = 0.027) |
Well tolerated
No serious adverse events
One urosepsis resulting in exclusion from the study
No difference in ADRs (P = 0.68)
No difference in trough levels of immunosuppressive drugs
No rejection episode |
| Schwaiger et al23 |
Significant effects: baseline vs. time after initiation mean (SD); P-value
Waist circumference (cm): 103.1 (14.4) vs. week-4: 99.1 (14.3); P = 0.001
Fluid volume overload (L): 2.7 (2.1) vs. week-4: 1.8 (1.8); P = 0.006
HbA1c (%): 6.7 (0.7) vs. month-12: 7.1 (0.8); P = 0.03
Magnesium (mmol/L): 0.70 (0.11) vs. month-12: 0.77 (0.11); P = 0.003
Waist circumference (cm): 109.7 (9.5) vs. month-12: 102.8 (7.1); P = 0.007
Weight (kg): 83.7 (7.6) vs. month-12: 78.7 (7.7); P = 0.02
BMI (kg/m2): 29.3 (3.1) vs. month-12: 27.7 (3.8); P = 0.04
DBP (mm Hg): 86 (14) vs month-12: 76 (11); P = 0.02
Uric acid (mg/dL), median (IQR): 7.5 (6.7-9.4) vs. week-4: 6.2 (5.9-7.1); P = 0.04 |
Baseline vs. week-4:
Significant decrease in eGFR (mean ± SD): baseline 55.6 ± 20.3 vs. 47.5 ± 15.1 mL/min/1.73 m2 on week-4; P = 0.008
Three cases of bacterial UTI
One uncomplicated balanitis
One hospitalization due to pneumonia
No cases of ketoacidosis
Therapy discontinuation between 4 weeks and 12 months: 6 patients
Baseline vs. month-12:
Bacterial UTI in 5 empagliflozin-treated patients and 9 non-receivers; P = 0.81 |
| Song et al32 |
Significant effects: baseline vs. 6 months after mean (SD); P-value
Weight (kg): −2.95 (3.54); P = < 0.0001 (95% CI: 3.53, 1.50)
Hypomagnesemia: 0.13 (1.73), P = 0.0004 (95% CI: 0.06, 0.20) |
UTI in 7 patients, mean days after initiation: 69.4 (non-significant)
No cases of ketoacidosis
No amputations
No AKI
Therapy discontinuation after ADR in 7 cases |
| Lim et al26 |
Significant effects: intervention vs. control log-rank P
Serum creatinine doubling: 0.009 |
All-cause mortality: 0.005
DCGF: 0.005
Acute dip of over 10% in 15.6% of the intervention group during the first month
A significant interaction between intervention initiation and time in eGFR within 8 months (P = 0.044) |
| Fructuoso et al.30 |
Significant effects: baseline vs. 6 months after mean (SD); P-value
Weight loss (kg): 83.9 (17.6) vs. 81.8 (17.2); P < 0.001
SBP (mm Hg): 137.2 (15.7) vs. 133.0 (15.9); P < 0.001
DBP (mm Hg): 76.7 (9.8) vs. 74.2 (9.8); P < 0.001
Hemoglobin (g/dl): 13.6 (1.7) vs. 14.1 (1.6); P < 0.001
Fasting glycaemia (mg/dl):152.8 (42.2) vs. 135.2 (37.2); P < 0.001)
HbA1c (%): 7.6 (1.2) vs. 7.12 (0.9); P < .001
eGFR (mL/min/1.73 m2): 60.2 (20.2) vs. 58.5 (20.9); P = 0.01
Uric acid (mg/dl): 6.2 (1.4) vs. 5.8 (1.3); P < 0.001
Magnesium (mg/dl): 1.6 (0.3) vs. 1.8 (0.3); P < 0.001
Significant effects: 6 months vs. 12 months after mean (SD); P-value
Weight (kg): 81.8 (17.2) vs. 80.6 (17.4); P < 0.001 |
6-months follow-up:
Pre-treatment UTI positive vs. negative: 35.6% vs. 6.5%; P < .001
Female vs. male UTI: 18.5% vs. 8.5%; P = 0.015
12-months follow-up:
Total ADRs: 26%
UTI: 14%
Polyuria: 4.7%
AKI: 1.8%
Genital mycosis: 1.5%
Hypoglycemia: 1.2%
Diarrhea: 0.6% |
| Maigret et al28 |
Significant effects: baseline vs. 3 months after median (IQR); P-value
SBP (mm Hg): 143 (132-155) vs. 138 (126-150); P < 0.0001
DBP (mm Hg): 81 (73-99) vs. 78 (69-85); P < 0.0001
eGFR (ml/min/1.73 m2): 43.8 (37.0-53.9) vs. 43.1 (34.1-53.1); P < 0.0001
Serum creatinine (µmol/L): 146 (116-174) vs. 152 (119-186); P < 0.0001
Proteinuria (mg/dL): 748 (312-1832) vs. 637 (276-1272); P = 0.0005
Significant effects: baseline vs. 6 months after median (IQR); P-value
SBP (mm Hg): 143 (132-155) vs. 140 (129-152); P = 0.022
DBP (mm Hg): 80 (72-89) vs. 78 (70-84); P = 0.001
eGFR (mL/min/1.73 m2): 45.1 (38.2-55.1) vs. 43.5 (35.9-53.6); P < 0.0001
Serum creatinine (µmol/L): 140 (112-172) vs. 147 (115-182); P < 0.0001
Proteinuria (mg/dL): 650 (315-1448) vs. 500 (270-1094); P = 0.006 |
12-months ADRs:
Graft dysfunction: 4.9%
Lower UTI: 4.6%
Pyelonephritis: 2%
Genital infection: 2%
Pulmonary infections: 8%
Digestive infections: 1.7%
Other infections: 3.7%
Digestive symptoms: 3.5%
Total ADRs leading to discontinuation: 15.6% (95% CI: 12.1– 20.2)
*Higher incidence of SGLT-2 inhibitor discontinuation in eGFR < 30 mL/min/1.73 m2 |
| Hisadome et al25 |
Significant effects: intervention vs. control mean difference (SD); P-value
Weight loss (kg): -7 (5.1) vs. 1.6 (4.5); P= 0.04 |
No significant differences:
UTIs
Biopsy-proven acute rejection |
| Sheu et al31 |
Significant effects: intervention vs. control aHR; P-value (95% CI)
All-cause mortality: 0.32; P < 0.001 (0.22–0.45)
MACE: 0.48; P < 0.001 (0.37-0.62)
MAKE: 0.52; P < 0.001 (0.43–0.62)
Dialysis frequency: 0.45 (95% CI: 0.32–0.63) |
Significant ADRs: intervention vs. control aHR (95% CI)
Diabetic ketoacidosis: 1.84 (1.06-3.20)
Osteoporosis fracture: 2.93 (1.16-7.43) |
| Gill et al24 |
NR |
Hematocrit base vs. 3 months after mean (SD):
Base: 31% (3.5), no cases ≥ 50%
3 months after: 42% (6), 5% cases ≥ 50%
In median follow-up of two years n (%):
Death: 2 (5)
Allograft failure: 2 (5)
Permanent drug discontinuation n (%):
Thrombotic events (stroke): 1 (2%)
Urosepsis: 2 (5%)
AKI: 2 (5%)
Low kidney allograft function: 1 (2%)
Hyponatremia: 1 (2%)
Surgical procedures: 2 (5%) |
| Mahling et al27 |
Baseline vs. after median follow-up of 12.0 months (IQR: 5.3, 12.0)
a:
Stable kidney allograft throughout the study (according to eGFR values)
HbA1c (%) median (IQR): 7.3 (6.4, 7.8) vs. 7.1 (6.6, 7.5)
Total daily insulin requirement (%): 10-25 lower
Body weight (kg) absolute change%: –1.9 (–1.9, 0.1)
Waist circumference (cm) absolute change%: –2.0 (–6.0, 0.0)
SBP (mm Hg) absolute change%: –2.5 (–36.3, 0.8)
DBP (mm Hg) absolute change%: –0.5 (–9.5, 7.5)
Hematocrit (%) absolute change%: + 2.5 (0.8, 4.1)
Uric acid (mg/dL) absolute change%: –0.2 (–0.8, 0.5) |
ADR n (%):
UTI: 2 (20)
AKI stage I: 1 (10)
Lower limb small diabetic ulcer: 1 (10)
No permanent decline in renal function
No urosepsis
No ketoacidosis
Drug discontinuation n (%):
Feeling more tired: 1 (10)
Respiratory tract infection and temporary allograft disfunction: 1 (10) |
| Quilis et al29 |
Significant effects: baseline vs. 6 months after median (IQR); P-value
UPCR (g/g): 1.68 (0.58, 2.9) vs. 1.06 (0.42, 1.65); P = 0.025
Uric acid (mg/dL): 7.2 (6.2, 8.5) vs. 6.6 (6.2, 7.5); P = 0.013
HDL (mg/dL): 58.5 (39, 61.5) vs. 48 (40, 59); P = 0.027
eGFR (mL/min/1.73 m2): 31 (23.7, 45.2) vs. 28.5 (19.7, 37.2); P = 0.001 |
Drug discontinuation n (%):
UTI: 1 (4.5)
Hemodialysis initiation: 1 (4.5)
No cardiovascular events
No deaths |
| Demir et al9 |
Non-significant effects: intervention vs. control; P-value
Proteinuria (mg/day) median (IQR): 195 (51–1905) vs. 156 (44–1355); P = 0.372
eGFR (ml/min/1.73 m2) mean (SD): 72.96 (16.62) vs.65.36 (17.19); P = 0.123
HgbA1c (%) mean (SD): 7.71 (1.25) vs. 7.14 (0.98); P = 0.256
Significant effect: SGLT-2 inhibitor baseline vs. 12 months after median (IQR); P-value
Proteinuria (mg/day): 321 (45–2565) vs. 195 (51–1905); P = 0.008 |
Non-significant ADRs: intervention vs. control
UTI (%): 16.67 vs. 28.57; P = 0.327
Hospitalization (%): 8.3 vs. 23.8; P = 0.105
Significant ADRs: intervention vs. control
Acute rejection episodes (%): 11.1 vs. 33.3: P = 0.040 |
| Cohen et al33 |
Non-significant effects: intervention vs. control HR (95% CI); P-value
All-cause mortality rate: 0.66 (0.38–1.14); P = 0.135
Composite renal outcome: 0.99 (0.65–1.52), P = 0.970)
Significant effect: SGLT-2 inhibitor baseline vs. 12 months after median (IQR); P-value
HbA1c (%): 7.7 (6.9–8.4) vs. 7.2 (6.8–7.9); P = 0.003 |
The risk of UTI hospitalization was significantly lower in the SGLT-2 inhibitor group (5.7 vs. 10.5 events/100 patient-years, HR 0.55, 95 % CI 0.34–0.89, P = 0.016)
The incidence of other safety outcomes was similar between the study groups |
| Shah et al38 |
Significant effects: baseline vs.6 months mean (SD); P-value
Weight (kg): 78.6 (12.1) vs. 76.2 (10.9); P < 0.05
SBP (mm Hg): 142 (21) vs. 134 (17); P < 0.05
HbA1C (%): 8.5 (1.5) vs. 7.6 (1); P < 0.05 |
No common side effects were reported;
No UTIs, mycotic infection, hypotension, orthostatic hypotension, hypoglycemia, or increased thirst |
| Miyazaki et al37 |
Changes before and after administration in 5 cases
a:
Weight (kg): decreased in 4/5
Waist circumference (cm): decreased in 4/5
SBP (mm Hg): decreased in 4/5
DBP (mm Hg): decreased in 3/5
Creatinine (mg/dL): increased in 3/5
eGFR (mL/min/1.732): decreased in 3/5
Uric acid (mg/dL): increased in 3/5
ALT (IU/L): decreased in 5/5
ℽ-GTP (IU/L): decreased in 5/5
TG (mg/dL): decreased in 4/5
HbA1c (%): decreased in 4/5
UACR (mg/g creatinine): decreased in 5/5 |
ADRs:
No AKI
No urogenital infection |
| Attallah et al35 |
Mean changes before and after administration in 8 cases
a:
Weight (kg): -2.4
HbA1c
Urine protein (g/day): -0.6 |
ADRs n (%):
Temporary nausea: 2 (25)
UTI: 2 (25)
No organ rejection |
| Gul et al36 |
Changes before and after administration in 4 cases
a:
Glycemic control improvement
Weigh (kg)/BMI: decreased in 4/4 |
ADRs n (%):
Genital/urinary infection: 1 (25)
No allograft dysfunction
No diabetic ketoacidosis |
| AlKindi et al34 |
Significant effect: baseline vs. 12 months after mean (SD); P-value
HbA1c (%): 9.34 (1.36) vs. 7.41 (1.44); P < 0.05
BMI (kg/m2): 32.74 (7.2) vs. 27.4 (4.2); P < 0.05 |
ADRs n (%):
Bacterial UTI: 1 (12.5)
No fungal infection |
| Sweiss et al42 |
Significant effects: baseline vs. nadir values 3-12-month after median (IQR); P-value
HbA1c (%): 8.0 (7-9) vs. 7 (6-8); P = 0.0005
FPG (mg/dL): 156 (116-211) vs. 118 (99-148); P < 0.0001
Weigh (kg): 88 (78-102) vs. 85 (76-100); P = 0.0003
BMI (kg/m2): 32 (27-34) vs. 31 (27-34); P = 0.0017 |
ADRs n (%):
Hypoglycemia: 10 (20)
Hypotension: 7 (14)
UTI: 1 (2)
Volume depletion: 4 (8)
Stroke: 1 (2) |
| Rajasekeran et al44 |
No significant changes over time in evaluated outcomes; HbA1c, weight, serum potassium, SBP, creatinine, or eGFR |
ADRs n (%):
No UTI
No mycotic infection
No AKI
Hypoglycemia without hospitalization: 1 (10)
Cellulitis: 1 (10) |
| Lemke et al45 |
Significant change in HbA1c (%) median (IQR); P-value:
Baseline to 3 months: -0.6 (-1.2, 0); P = 0.013
Baseline to 12 months: -0.4 (-1.4, 0.1); P = 0.016 |
ADRs n (%):
UTI: 6 (15)
Diabetic foot ulcers: 2 (5)
Mild hypoglycemia: 2 (5)
Hospitalization for diabetic ketoacidosis and concurrent UTI: 1 (3%)
AKI: 2 (5)
Intervention discontinuation: 17 (43%) |
| Muir et al41 |
Significant effects: baseline vs. after ≥ 3 months mean (SD); P-value:
Weight (kg): 89.2 (15.4) vs. 86.5 (16.1); P = 0.05
BMI (kg/m2): 29.8 (4.2) vs. 28.9 (4.5); 0.04
SBP (mm Hg): 134 (16) vs. 122 (16); P = 0.03
DBP (mm Hg): 82 (11) vs. 75 (11); P = 0.03
Furosemide dose (mg): 45 (76) vs. 16 (43); P = 0.05 |
ADRs n (%):
Dizziness: 1 (5)
UTI exacerbation and polyuria: 1 (5) |
| Cehic et al40 |
Significant effects: baseline vs. after 12 months median (IQR); P-value
Weight (kg): 90.1 (82.3, 101.9) vs. 88.1 (76.2, 96.6); P = 0.003
BMI (kg/m2): 30.5 (26.7, 32.7) vs. 29.2 (24.1, 31.5); 0.004
Furosemide dose (mg): 20 (0, 80) vs. 0 (0, 0); P = 0.02 |
ADRs n (%):
Exacerbation of urinary symptoms: 1 (4)
Dizziness: 1 (4)
AKI (leading to cessation): 1 (4)
No genitourinary infections. |
| Marfella et al39 |
Significant effects among diabetic patients: intervention vs. comparison mean (SD); P-value
HOMA-IR: 4.81 (0.66) vs. 5.61 (0.49); P < 0.01
Significant effects among intervention group: baseline vs. 12 months after mean (SD); P-value
HbA1c (%):6.54 (0.67) vs. 5.91 (0.98); P = 0.011
HOMA-IR: 4.47 (0.37) vs. 4.81 (0.66); P = 0.038
Cholesterol (mg/dL): 176.1 (18.3) vs. 159.7 (33.7); P = 0.025
Triglycerides (mg/dL): 190.9 (27.8) vs. 162.1 (20.3); P = 0.004 |
NR
|
| Mahmoud et al43 |
Significant effects: baseline vs. after treatment P-value
HbA1c (%) reduction: P < 0.0001
BMI (kg/m2) reduction: P = 0.0089 |
ADRs n (%):
Myocardial infarction: 2 (2)
Heart failure: 1 (1)
Cerebrovascular accidents: 1 (1)
UTI: 15 (15)
Genital infection: 1 (1) |
ℽ-GTR, ℽ-Glutamyl Transpeptidase; ADR, Adverse Drug Reaction; AKI, Acute Kidney Injury; ALT, Alanine Aminotransferase; BMI, Body Mass Index; DBP, Diastolic Blood Pressure; DCGF, Death-Censored Graft Failure; eGFR, estimated Glomerular Filtration Rate; FPG, Fasting Plasma Glucose; HbA1c, Hemoglobin A1c; HDL, High-Density Lipoprotein; HOMA-IR, homeostatic model assessment for insulin resistance; IQR, interquartile range; IRS-1, Insulin receptor substrate 1; IRS-2, Insulin receptor substrate 2; LDL, Low-Density Lipoprotein; MACE, Major Adverse Cardiac Events; MAKE, Major Adverse Kidney Events; NR, Not Reported; OGTT, Oral Glucose Tolerance Test; PPAR-γ, peroxisome proliferator-activated receptor gamma; SBP, Systolic Blood Pressure; SD, Standard Deviation; SGLT-2, Sodium-Glucose Transporter 2; TG, Triglyceride; UACR, Urinary Albumin-to-Creatinine Ratio; UTI, Urinary Tract Infection; VAT, Visceral Adipose Tissue
a Data regarding the significance of the results were not reported in this study.
Kidney transplant
Interventional studies
Two interventional studies including 58 individuals were carried out to evaluate the effects of empagliflozin 10 mg/d in patients with stable kidney transplants.22,23 Halden et al, in an investigator-initiated, single-center, prospective, double-blind study of 44 patients with NODAT, at least 12 months following transplantation, and stable renal function (less than a 20% deviation in serum creatinine [SrCr] within the last two months) showed that empagliflozin significantly improved hemoglobin A1c (HbA1c) (P = 0.025), body mass index (BMI) (P= 0.011), body weight (P = 0.014), uric acid (P < 0.001), hemoglobin (P = 0.047), and hematocrit (P = 0.027) with no clinical effects on immunosuppressive drug levels as well as comparable adverse event profile to placebo. There were no significant differences between the study groups regarding fasting plasma glucose (FPG), 2-hour glucose after oral glucose tolerance test (OGTT); waist-hip ratio, mean 24-hour systolic blood pressure (SBP); mean 24-hour diastolic blood pressure (DBP), and estimated glomerular filtration rate (eGFR). Notably, magnesium levels were significantly higher in the intervention group compared to placebo (P < 0.01).22
Schwaiger et al, in a non-inferiority pilot study, included 14 patients with NODAT who were on insulin therapy (less than 40 IU per day), with eGFR ≥ 30 mL/min per 1.73 m2, during at least six months post-transplantation, aiming at replacing their insulin therapy to 10 mg empagliflozin per day. According to their results, empagliflozin could significantly decrease body weight (P = 0.02), BMI (P = 0.0), fluid volume overload (P = 0.006), waist circumference (P = 0.007), uric acid (P = 0.04), and DBP (P = 0.02) OGTT–derived 2‐hour glucose measurement as the primary outcome showed an increase from 232 ± 82 mg/dL (baseline) to 273 ± 116 mg/dL (after 4 weeks, P = 0.06) and to 251 ± 71 mg/dL (after 12 months, P= 0.41). Similar to the Halden et al study, administration of empagliflozin led to a significant increase in magnesium levels (P < 0.01).23
Efficacy data in interventional studies
Our meta-analysis revealed that empagliflozin 10 mg/d could significantly decrease BMI (-2.564, 95% CI: -4.982 to -0.146, I2 = 0%, P = 0.0377), weight (-0.800, 95% CI: -0.878 to -0.722, I2 = 0%, P< 0.0001) and HbA1c (-0.447, 95% CI: 0.085 to 0.810; I2 = 0%, P = 0.0155); whereas uric acid did not reduce significantly (-26.655, 95% CI: -77.310 to 24.001; I2 = 97.54%, P = 0.3024). The detailed results and corresponding forest plots are shown in Figure 4A-4D.
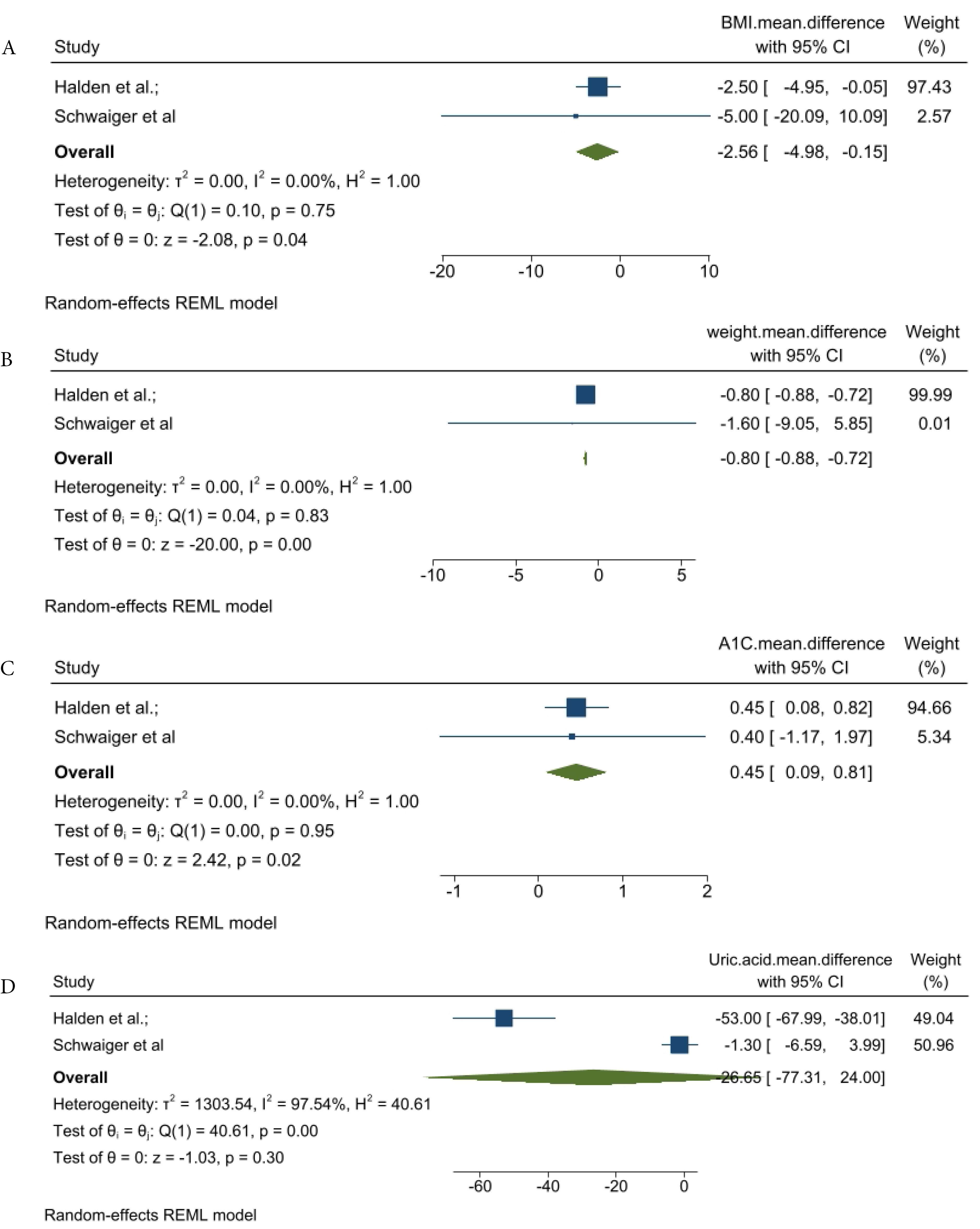
Figure 4.
Generated Forest plots for the meta-analysis. A) Forest plots for changes in body mass index B) Forest plots for changes in weight C) Forest plots for changes in hemoglobin A1c D) Forest plots for changes in uric acid
.
Generated Forest plots for the meta-analysis. A) Forest plots for changes in body mass index B) Forest plots for changes in weight C) Forest plots for changes in hemoglobin A1c D) Forest plots for changes in uric acid
Safety data in interventional studies
In Halden et al RCT, one patient in the empagliflozin group was withdrawn from the study due to urosepsis.22 There was no significant difference between the study groups regarding the reported total adverse events (P= 0.68). No case of rejection episode was reported. In addition, eGFR was significantly reduced in the empagliflozin group after eight weeks (-4 [-7, -1] mL/min/1.73 m2 vs. -1 [-2, 2] mL/min/1.73 m2; P < 0.05); however, no difference in change in eGFR between the study groups was observed (P = 0.61), reflecting a temporary decline in eGFR.
In Schwaiger et al interventional non-inferiority pilot study, empagliflozin administration led to a significant decrease in eGFR (55.6 ± 20.3 at the baseline vs. 47.5 ± 15.1 mL/min per 1.73 m2 at the fourth week; P = 0.008).23 From baseline to week four, three cases of bacterial UTI, one uncomplicated balanitis, and one hospitalization due to pneumonia were observed. No case of ketoacidosis occurred. During the follow-up of 12 months, bacterial UTI occurred in five empagliflozin‐treated patients, and in nine out of 24 patients from the untreated reference group (P = 0.81).
Observational studies
A total of 12 observational studies involving 7,463 participants were included to evaluate the potential effects of SGLT-2 inhibitors in kidney transplant patients.9,24-34 In a multi-center retrospective study by Lim et al, among 2,083 kidney transplant patients with type 2 DM, 226 were prescribed SGLT-2 inhibitors for at least 90 days.26 Over a mean follow-up duration of 62.9 ± 42.2 months, the administration of SGLT-2 inhibitors significantly reduced all-cause mortality (log-rank P = 0.005), Death-Censored Graft Failure (DCGF) (log-rank P = 0.005), and SrCr doubling (log-rank P = 0.009).
Sheu et al utilized the TriNetX database to assess the impact of SGLT-2 inhibitors on all-cause mortality, major adverse cardiac events (MACE), and major adverse kidney events (MAKE).31 After propensity score matching of 1970 SGLT-2 inhibitor users with non-users, the results revealed that the use of SGLT-2 inhibitors can significantly decrease all-cause mortality (adjusted hazard ratio [aHR] = 0.32), MACE (aHR = 0.48), and MAKE (aHR = 0.52) over a median follow-up of 3.4 years.31
Cohen et al conducted a retrospective analysis involving 240 kidney transplant patients with DM using SGLT2 inhibitors and 240 non-users.33 The study found that SGLT2 inhibitor users had a lower incidence of composite renal outcomes (8.9 vs. 13.3 events per 100 patient-years). However, after adjusting for independent predictors, the risk was similar (HR = 0.99, 95% CI: 0.65–1.52, P = 0.970), and there was no significant difference in all-cause mortality (HR = 0.66, 95% CI: 0.38–1.14, P = 0.135). Importantly, HbA1c levels decreased significantly from 7.7% to 7.2% after one year of SGLT2 treatment (P = 0.003) and remained stable over the following two years.
Based on the Quilis et al study on 22 non-diabetic patients, the use of SGLT-2 inhibitors led to a significant decrease in proteinuria (1.68 to 1.06 g/g, P = 0.025), uric acid (7.2 to 6.6 mg/dL, P.013), high-density lipoprotein (HDL) (58.5 to 48 mg/dL, P = 0.027), and eGFR (31 to 28.5 mL/min, P = 0.001) with no cardiovascular adverse events or death.29
In Maigret et al’s prospective multicenter real-life study, SGLT-2 inhibitors were associated with a significant improvement in proteinuria, blood pressure (BP), and eGFR in diabetic and non-diabetic kidney transplant patients (all P < 0.01).28 In Demir et al retrospective observational study of 57 patients with diabetes and kidney transplants, the use of an SGLT-2 inhibitor resulted in a significant improvement in proteinuria (P= 0.008). Interestingly, the eGFR initially declined from a baseline of 71.94 ± 18.17 ml/min/1.73 m2 to 68.36 ± 19.98 ml/min/1.73 m2 by the third-month post-transplant. However, by 12 months post-transplant, the eGFR increased to 72.96 ± 16.62 ml/min/1.73 m2 in patients who received the SGLT-2 inhibitor.9
The remaining studies were mainly focused on metabolic outcomes. Song et al performed a single-center retrospective analysis of 50 kidney transplant patients with pre-existing type 2 diabetes mellitus (T2DM) or NODAT and an eGFR of 30 mL/min or greater.32 This study indicated that SGLT-2 inhibitors could lead to an average weight loss of 2.95 kg (SD = 3.54; P< 0.0001; CI: 3.53 to 1.50) and ameliorate hypomagnesemia by 0.13 (SD = 1.73; P = 0.0004; CI: 0.06 to 0.20).
Hisadome et al conducted a retrospective observational study using inverse probability of treatment weighting to compare the effects of SGLT-2 inhibitors on changes in HbA1c, body weight, and eGFR after kidney transplantation with other hypoglycemic agents in 85 T2DM patients.25 The analysis revealed no significant differences between the groups in terms of changes in HbA1c; however, body weight significantly decreased in the SGLT-2 inhibitor group compared to the control group (−0.7 kg vs. + 1.6 kg; P = 0.040).
In a prospective observational study by Mahling et al, 10 patients with NODAT or T2DM and eGFR greater than 45 mL/min/1.73 m2 were assessed.27 The study showed that empagliflozin could reduce the median HbA1c from 7.3% to 7.1%.
In AlKindi et al study of 8 patients, the administration of SGLT-2 inhibitors led to a significant improvement in HbA1c and BMI (P < 0.05).34 In Fructuoso et al multi-center retrospective cohort study, over a six-month study period, the administration of SGLT-2 inhibitors led to significant improvements in weight, SBP, DBP, hemoglobin, fasting glycemia, HbA1c, and serum magnesium levels (all P values < 0.001).30
Safety data in observational studies
Two studies were conducted to investigate the safety profile of SGLT-2 inhibitors in kidney transplant patients. In a multi-center retrospective study by Fructuoso et al, the safety of SGLT-2 inhibitors was evaluated in 339 kidney transplant patients with pre-existing T2DM or NODAT as the primary outcome.30 The results revealed that adverse effects were reported in 26% of patients, with UTIs being the most common (14%). In 10% of cases, SGLT-2 inhibitors were discontinued primarily due to UTIs. Risk factors for developing a UTI included a prior episode of UTI within the six months preceding SGLT-2 inhibitor use (odds ratio [OR] = 7.90; CI: 3.63–to 17.21) and female sex (OR = 2.46; CI: 1.19 to 5.03). A post hoc subgroup analysis indicated that the incidence of UTIs was similar in diabetic kidney transplant recipients (DKTRs) treated with SGLT-2 inhibitors for 12 months compared to non-DKTRs (17.9% versus 16.7%). It has been also shown that SGLT-2 inhibitors could significantly improve eGFR over six months.
In Gill et al study on 42 patients with a mean eGFR of 71 mL/min/1.73 m2, the administration of SGLT-2 inhibitors resulted in a sustained increase in hematocrit three months after the treatment.24 Hematocrit levels of 50% or higher were observed in 10% of the patients, and one patient experienced a thrombotic event, which could not be conclusively linked to the increase in hematocrit.
In remaining observational studies, the safety of SGLT-2 inhibitors in kidney transplant patients was also reported. In the Lim et al study, adverse events were compared between the SGLT-2 inhibitor and non-SGLT-2 inhibitor groups.26 Notably, 15.6% of patients on SGLT-2 inhibitors experienced an acute dip of over 10% in eGFR during the first month. The earlier use of SGLT-2 inhibitor after kidney transplantation and higher mean tacrolimus trough level were independent risk factors for eGFR dip (time from kidney transplantation to SGLT-2 inhibitors usage: adjusted OR = 0.97, 95% CI: 0.95 to 0.99, P = 0.024; mean tacrolimus trough level: adjusted OR = 1.86, 95% CI: 1.11 to 3.11, P = 0.019).
In Song et al study, no cases of diabetic ketoacidosis, amputations, or AKI were reported during the six-month follow-up period.32 UTIs occurred in 14% of the patients, which was comparable to the rate in the high-risk population. Therapy discontinuation occurred in nine patients due to UTIs (n = 5), genital yeast infection (n = 1), native disease recurrence (n = 1), NODAT (n = 1), and physician preference (n = 1).
In the Hisadome et al study, there was no significant difference between SGLT-2 inhibitors and other hypoglycemic agents regarding eGFR, acute rejection, and other safety outcomes such as the incidence of UTIs (P = 0.106).25 One case of biopsy-proven acute rejection in each group was observed (P = 0.329). In the Demir et al study, there was no significant difference between SGLT-2 inhibitor and no SGLT-2 inhibitor groups regarding the incidence of UTI and UTI-related hospitalization, eGFR, HgbA1c levels, and weight during the study follow-up period of 12-month.9
In Mahling et al study, the rates of UTIs and other side effects were found to be low.27 Two cases of UTI (annual incidence of 0.32/patient/year) and one AKI stage I (0.16/patient/year) were observed among 10 empagliflozin-treated patients. The median eGFR at baseline was 57 mL/min/1.73 m2, which remained stable throughout the 12-month follow-up period (5.3 to 12.0 months). No case of urosepsis nor ketoacidosis was observed.
In Maigret et al study, the incidence of UTIs (6.6%) and genital mycosis (0.6%) were found to be low with no serious adverse event.28 SGLT-2 inhibitor discontinuation occurred in 15.6% of patients which was due to graft dysfunction, recurrent infections, UTI, and digestive symptoms. Notably, low eGFR, especially those with eGFR < 30 mL/min per 1.73 m2, seems to be a risk factor for the incidence of SGLT-2 inhibitors’ discontinuation (P = 0.003).
It is worth mentioning that in Sheu et al study, initiation of SGLT-2 inhibitors within three months of kidney transplant did not lead to a significant increase in any genitourinary infection, including UTI and candidiasis, (aHR = 1.03, 95% CI: 0.32 to 0.63) and AKI (aHR = 0.95, 95% CI: 0.85 to 1.07).31 Notably, in the Cohen et al study, the risk of UTI hospitalization was significantly lower in the SGLT2 inhibitor group (5.7 vs. 10.5 events/100 patient-years, HR = 0.55, 95 % CI: 0.34–0.89, P = 0.016). Notably, other safety outcomes were similar between the groups, reinforcing the potential of SGLT2 inhibitors as a safer treatment option.33
Case series
The potential effects of SGLT-2 inhibitors in kidney transplant patients have been evaluated in five case series.35-38 In a prospective study by Shah et al, 25 patients with pre-existing T2DM (80%) or NODAT (20%) and eGFR greater than 60 mL/min were treated with canagliflozin at a dosage of 100 mg/d.38 This treatment resulted in significant improvements in body weight (from 78.6 ± 12.1 kg before treatment to 76.2 ± 10.9 kg after treatment, P < 0.05), mean SBP (from 142 ± 21 mm Hg to 134 ± 17 mm Hg, P < 0.05), and HbA1c levels (from 8.5 ± 1.5% to 7.6 ± 1%, P< 0.05). There were no significant adverse events; however, DBP, SrCr, creatinine clearance, and tacrolimus levels did not show significant changes during the follow-up period of over six months.
In the study by Attallah et al, the effects of empagliflozin 25 mg/day were assessed in eight kidney transplant patients with T2DM or NODAT.35 The patients were followed for an average of 12 months. Results indicated that empagliflozin decreased body weight and HbA1c within the first three months, with these improvements sustained thereafter. Additionally, the average urine protein excretion was decreased by 0.6 g/day. However, one patient discontinued the medication due to recurrent UTIs.
Miyazaki et al evaluated the effects of empagliflozin at a dose of 10 mg/day in five non-diabetic renal transplant recipients with CKD stage G3a-4 and metabolic syndrome.37 Empagliflozin administration provided benefits regarding metabolic parameters, such as weight, waist circumference, HbA1c, and BP, in four out of the five cases, with no adverse events reported.
In the study conducted by Gul et al, the administration of empagliflozin at 10 mg/day in four patients with T2DM or NODAT resulted in the loss of 2-3% of body weight in all patients, without causing any deterioration in allograft function or interfering with the pharmacokinetics of immunosuppressant medications.36 However, one case of genital/urinary infection was reported.
Other solid transplants
Marfella et al performed a study on the pathogenesis of experimental diabetic cardiomyopathy involving 70 heart transplant patients over a period of 12 months.39 The biopsy results revealed a progressive increase in the cardiac expression of JunD/peroxisome proliferator-activated receptor-γ and ceramide levels, along with a notable decrease in insulin receptor substrates 1 and 2 in diabetic heart transplant patients. Interestingly, these molecular changes were less pronounced in patients with diabetes who were receiving SGLT2 inhibitors.
The effects of empagliflozin in patients with heart transplants who had NODAT or pre-existing T2DM were assessed in a retrospective single-center observational study. The results were reported in two separate studies, Muir et al and Cehic et al, including the results for three and 12 months of follow-up, respectively.40,41
In the Muir et al study, adding empagliflozin 10 mg (52.6%) or 25 mg (47.4%) to the therapeutic regimen resulted in significant improvements in body weight (2.7 ± 5.1 kg decrease, P = 0.05), BMI (reduced by 0.9 ± 1.7 kg/m2, P= 0.04), SBP (decreased by 12 ± 19 mm Hg, P = 0.03), and DBP (reduced by 7 ± 11 mm Hg, P = 0.03).41 However, there was no significant reduction in HbA1c levels. One patient reported polyuria and exacerbation of pre-existing lower urinary tract symptoms.
Accordingly, the study by Cehic et al, also indicated that empagliflozin 10 mg (45.45%) and 25 mg (54.55%) is safe for heart transplant recipients.40 There were three adverse events recorded in patients treated with empagliflozin (n = 20), leading to treatment discontinuation in one case. Notably, there were no genitourinary tract infections reported in the empagliflozin-treated group, while nine urinary infections occurred in the non-empagliflozin group (n = 77), who were receiving other anti-diabetic medications. Over 12 months, empagliflozin significantly reduced body weight (baseline: 90.1 kg [82.3–101.9] vs. month 12: 88.1 kg [76.2–96.6], P = 0.003) and BMI (baseline: 30.5 kg/m2 [26.7–32.7] vs. month 12: 29.2 kg/m2 [24.1–31.5], P = 0.004), but no significant changes were seen in HbA1c, SBP, DBP, urea, SrCr, or eGFR.
In a single-center, retrospective program evaluation study conducted by Sweiss et al, 41 diabetic patients were analyzed.42 The participants included 26 liver transplant recipients, 18 kidney transplant recipients, 4 lung transplant recipients, and 1 individual who received a simultaneous liver-kidney transplant. The SGLT2 inhibitor administration led to a significant improvement in HbA1c (P = 0.0005), fasting blood glucose (P ≤ 0.001), body weight (P = 0.0003), and BMI (P = 0.0017) during the follow-up period of 12 months. No patient experienced myocardial infarction, graft loss, or mortality during the 3 to 12-month period. There was one reported case each of UTI and stroke.
Mahmoud et al conducted a retrospective single-center observational study to evaluate the efficacy and safety of canagliflozin (100–300 mg daily) in liver transplant patients with NODAT or T2DM over a follow-up period of 12 months.43 The patients were at least three months post-transplant and had a minimum eGFR of 25 mL/min/1.73 m2. The HbA1c level decreased by 0.4% in the SGLT-2 inhibitor group (P< 0.0001), while the control group showed no significant changes ( + 0.05%; P = 0.2578). BMI reduction over the year was significant in the SGLT-2 inhibitor group (P = 0.0089) compared to the control group. Moreover, a significant reduction in albuminuria was observed in the SGLT-2 inhibitor group (P < 0.0001). No statistical differences were found regarding SBP and DBP between the two groups. One patient in the SGLT-2 inhibitor group developed a single episode of candida vulvitis, which was resolved with treatment after a temporary hold on the medication. In the SGLT-2 inhibitor group, 15 patients experienced a total of 34 episodes of UTIs, while 19 patients in the control group experienced a total of 39 UTI episodes. There was no significant difference in the median frequency of UTIs per patient between the study groups (P = 0.1325).
In a retrospective observational cohort study by Rajasekeran et al, which included 10 patients with simultaneous kidney-pancreas transplants or kidney transplants, and T2DM or NODAT, administration of canagliflozin resulted in overall but non-significant improvements in HbA1c, weight, SBP, and SrCr along with good safety profiles.44
Lemke et al conducted a retrospective descriptive study using electronic medical records, which showed that the administration of SGLT-2 inhibitors (dapagliflozin [61%], canagliflozin [31%], or empagliflozin [8%]) led to significant improvements in HbA1c at three (P = 0.013) and 12 months (P = 0.016).45 However, no clinically significant effects on SrCr or eGFR were observed in patients with type 2 DM or NODAT who underwent kidney, simultaneous kidney-pancreas, or simultaneous liver-kidney transplants.
Discussion
The present systematic review and meta-analysis provided an update on currently available evidence regarding the use of SGLT2 inhibitors in SOT recipients regardless of diabetes status. According to our results, the studies to date have been mostly conducted in kidney transplant populations, followed by heart, liver, and multi-organ transplantation.
The potential effects of SGLT-2 inhibitors in individuals with SOT have been evaluated in the Lin et al review, including 17 studies and emphasizing the need for further well-designed research focusing on the effects of SGLT-2 inhibitors on clinically significant outcomes, such as mortality reduction.14 These outcomes have been addressed in additional studies that are included in our systematic review and meta-analysis.
In a scoping review by Mreyoud et al involving 20 studies, it was found that SGLT-2 inhibitors reduce HbA1c levels and may contribute to weight loss in patients with SOT.46 However, they noted that cardiovascular and kidney outcomes were not adequately assessed in the reviewed studies. Our systematic review and meta-analysis revealed statistically significant effects of SGLT-2 inhibitors on both HbA1c and body weight. It is important to note that our eligibility criteria differed from those of Mreyoud et al and Lin et al; for instance, we excluded letters and case reports from our study. In addition, the present study is the most comprehensive systematic review of SGLT-2 inhibitors in SOT to date, including the most recent studies that were not included in the previous reviews.24,28,29,31,33
Efficacy
The meta-analysis of two available interventional studies revealed the short-term beneficial effects of SGLT-2 inhibitors on weight, BMI, and HgA1c in kidney transplantation patients. Our study also supported the beneficial effects of SGLT-2 inhibitors on metabolic outcomes in most eligible non-interventional studies in the SOT population, which aligns with previous studies in patients with T2DM, HF, or CKD.47-49
SGLT2 inhibitors could lower BP through several potential mechanisms, including weight loss, diuresis, decreases in plasma volume, and inhibition of the sympathetic nervous system.50 A network meta-analysis showed that SGLT2 inhibitors reduced SBP and DBP by −2.89 (95% CI: −3.37 to −2.40) mm Hg and −1.44 (95% CI: −1.68 to −1.2) mm Hg in adults with T2DM, respectively.51 Similar findings have been observed in other populations, such as patients with cardiovascular diseases.52,53 A systematic review and meta-analysis of 16 RCTs showed that SGLT2 inhibitors could significantly reduce SBP by 1.68 mm Hg (P = 0.001) in individuals with HF.54 Comparably, based on the findings of our study, SGLT-2 inhibitors could potentially improve BP control.
In the past decade, several real-world studies and RCTs have shown the mortality benefits of SGLT2 inhibitors in individuals with T2DM, HF, or CKD. Based on the robust evidence from a meta-analysis of 13 trials including 90,413 individuals, SGLT2 inhibitors significantly reduced cardiovascular death by 16% in HF, 15% in T2DM, and 12% in CKD.55 Based on our systematic review, the mortality benefits of SGLT-2 inhibitors in individuals with kidney transplantation have been observed in two observational studies. One multi-center retrospective cohort study including 2083 individuals with kidney transplants showed that SGLT2 inhibitors could improve all-cause mortality, DCGF, and serum creatinine.26 Another observational study showed that SGLT-2 inhibitors could significantly lower all-cause mortality, MACE, and MAKE.31 In the retrospective study by Cohen et al, there was no significant difference in all-cause mortality between the SGLT-2 inhibitor and the control group (HR = 0.66, 95% CI: 0.38–1.14, P= 0.135).33
Safety
SOT recipients are more vulnerable to infection-related mortality. It has been shown that infections account for 13% to 16% of the deaths in kidney and heart transplant recipients and up to 21% in lung transplant recipients.56 It is well known that immunosuppressive treatment used commonly in individuals with SOT is related to a high infection risk and the glycosuria induced by SGLT2 inhibitors may promote bacterial and fungal growth.57,58
UTIs occurred in the majority of the studied population, in which the rate of UTI was comparable with the high-risk population. It is worth mentioning that in the Sheu et al study with a large sample size and long follow-up duration, initiation of SGLT-2 inhibitors within 3 months of kidney transplant did not lead to a significant increase in any genitourinary infections.31 Interestingly, it has been shown that SGLT-2 inhibitors could even decrease UTI hospitalization in individuals with kidney transplantation.33 However, due to the complications of UTI such as impaired graft function, graft loss, and death in SOT patients, SGLT-2 inhibitors should be used with caution in this population.
Based on the literature, individuals with SOT are predisposed to kidney damage due to their clinical conditions and the use of nephrotoxic medications.59 Besides, SGLT2 inhibitors can potentially predispose individuals to AKI by causing volume depletion, which is attributed to their natriuretic properties and influence on tubuloglomerular feedback.47 It is worth mentioning that some medications can be continued even if there is a decrease in the eGFR, and certain medications may be resumed while AKI is still ongoing. This situation underscores the necessity of having a thorough understanding of drug-induced kidney damage.60 Research has shown that SGLT2 inhibitors may initially cause a decrease in eGFR, which typically stabilizes after a few weeks. This temporary decline in eGFR, observed after starting SGLT2 inhibitors, reflects the therapeutic hemodynamic mechanism of these medications as they reduce intraglomerular pressure and hyperfiltration, which is labeled as “permissive AKI” or “permissive hypercreatinemia”.61,62 Similar findings were observed in our study for individuals with SOT. Importantly, this early decrease does not negate their long-term protective effects on kidney function. In line with this, the beneficial effects of SGLT-2 inhibitors on MAKE and proteinuria have been observed in the kidney transplant population.28,29,31
Calcineurin inhibitors carry a significant risk of toxicity to the kidneys, which can lead to a heightened chance of advancing renal insufficiency in patients with SOT.63 Notably, in kidney transplant patients, calcineurin inhibitors have shown to downregulate the TRPM6 magnesium channel in the distal collecting tubule, resulting in hypomagnesemia that accelerates the decline of allograft function and further exacerbation of DM, CKD, hypertension, cardiovascular risks, and post-transplant osteoporosis.64-66 So, elevated magnesium levels after using SGLT-2 inhibitors may reduce adverse events related to calcineurin inhibitors.
SGLT-2 inhibitors can have beneficial effects in managing drug-induced nephrotoxicity. Based on Botros et al study on rats, empagliflozin could protect against gentamycin-induced nephrotoxicity by decreasing gentamicin concentration in renal tissue and its antioxidant and antiapoptotic properties. Moreover, the daily dose of 20 mg/kg empagliflozin may lead to renal tubular regeneration.67 Similar findings have been observed in the clinical studies. A recent meta-analysis of 12 studies found that SGLT-2 inhibitors significantly reduced contrast-induced nephrotoxicity (P < 0.0001) and mortality (P = 0.0039).68 Given these findings, the potential benefits of SGLT-2 inhibitors in the context of nephrotoxicity caused by calcineurin inhibitors warrant further investigation in future studies.
Limitations
The findings of this systematic review and meta-analysis should be interpreted with caution due to the following limitations: First, despite the suggested mechanisms of action, clinical data is insufficient to draw clear conclusions regarding the efficacy and safety of SGLT2 inhibitors in patients with SOT. Second, there was significant heterogeneity between included studies regarding the design, setting, sample size, population, duration of diabetes, time to SGLT2 inhibitor initiation post-transplantation, type, daily dose, and treatment duration of SGLT-2 inhibitors, and outcomes. Most studies have focused on patients who have undergone kidney organ transplantation, which limits the applicability of clinical judgment to other types of SOTs. Additionally, it’s important not to overlook the presence of multiple confounding factors, such as the lack of a control group in some studies, underlying health conditions, and concurrent medications. For example, many studies did not take into account potential confounders like diabetes and the specific types of immunosuppressive medications used. Moreover, non-interventional studies were not included in the meta-analysis due to their heterogeneity. Finally, due to the differences in study designs of interventional studies, data from their control groups were omitted from the meta-analysis.
Conclusion
The observational studies have shown the significant benefits of SGLT-2 inhibitors on clinical outcomes, including mortality, in kidney transplant patients. However, the field urgently needs well-designed RCTs to reinforce these findings. The majority of eligible studies clearly have established the beneficial effects of SGLT-2 inhibitors on metabolic outcomes in patients with SOT. Despite their generally acceptable safety profile in kidney transplant recipients, these medications must be used with caution, applying close monitoring and patient education, particularly in high-risk patients (e.g. previous episode of UTI or female sex). Additional well-designed studies with large sample sizes and longer follow-up periods are needed to evaluate the efficacy and safety of SGLT-2 inhibitors in individuals with kidney transplants and other SOT.
Competing Interests
The authors declare that they have no conflict of interest.
Ethical Approval
Not applicable.
Supplementary Files
Supplementary file 1 contains Table S1.
(pdf)
References
- Rana A, Gruessner A, Agopian VG, Khalpey Z, Riaz IB, Kaplan B. Survival benefit of solid-organ transplant in the United States. JAMA Surg 2015; 150(3):252-9. doi: 10.1001/jamasurg.2014.2038 [Crossref] [ Google Scholar]
- Sen A, Callisen H, Libricz S, Patel B. Complications of solid organ transplantation: cardiovascular, neurologic, renal, and gastrointestinal. Crit Care Clin 2019; 35(1):169-86. doi: 10.1016/j.ccc.2018.08.011 [Crossref] [ Google Scholar]
- Cowie MR, Fisher M. SGLT2 inhibitors: mechanisms of cardiovascular benefit beyond glycaemic control. Nat Rev Cardiol 2020; 17(12):761-72. doi: 10.1038/s41569-020-0406-8 [Crossref] [ Google Scholar]
- Chen J, Jiang C, Guo M, Zeng Y, Jiang Z, Zhang D. Effects of SGLT2 inhibitors on cardiac function and health status in chronic heart failure: a systematic review and meta-analysis. Cardiovasc Diabetol 2024; 23(1):2. doi: 10.1186/s12933-023-02042-9 [Crossref] [ Google Scholar]
- Herrington WG, Staplin N, Agrawal N, Wanner C, Green JB, Hauske SJ. Long-term effects of empagliflozin in patients with chronic kidney disease. N Engl J Med 2025; 392(8):777-87. doi: 10.1056/NEJMoa2409183 [Crossref] [ Google Scholar]
- Anderegg MA, Schietzel S, Bargagli M, Bally L, Faller N, Moor MB. Empagliflozin in nondiabetic individuals with calcium and uric acid kidney stones: a randomized phase 2 trial. Nat Med 2025; 31(1):286-93. doi: 10.1038/s41591-024-03330-x [Crossref] [ Google Scholar]
- Androutsakos T, Nasiri-Ansari N, Bakasis AD, Kyrou I, Efstathopoulos E, Randeva HS. SGLT-2 inhibitors in NAFLD: expanding their role beyond diabetes and cardioprotection. Int J Mol Sci 2022; 23(6):3107. doi: 10.3390/ijms23063107 [Crossref] [ Google Scholar]
- Khiali S, Taban-Sadeghi M, Sarbakhsh P, Khezerlouy-Aghdam N, Rezagholizadeh A, Asham H. SGLT2 inhibitors’ cardiovascular benefits in individuals without diabetes, heart failure, and/or chronic kidney disease: a systematic review. J Clin Pharmacol 2023; 63(12):1307-23. doi: 10.1002/jcph.2311 [Crossref] [ Google Scholar]
- Demir ME, Özler TE, Merhametsiz Ö, Sözener U, Uyar M, Ercan Z. The results of SGLT-2 inhibitors use in kidney transplantation: 1-year experiences from two centers. Int Urol Nephrol 2023; 55(11):2989-99. doi: 10.1007/s11255-023-03645-7 [Crossref] [ Google Scholar]
- Azadi S, Azarpira N, Roozbeh J, Ezzatzadegan-Jahromi S, Raees-Jalali GA, Foroughinia F. Genetic polymorphisms of glucocorticoid receptor and their association with new-onset diabetes mellitus in kidney transplant recipients. Gene 2023; 856:147138. doi: 10.1016/j.gene.2022.147138 [Crossref] [ Google Scholar]
- Ujjawal A, Schreiber B, Verma A. Sodium-glucose cotransporter-2 inhibitors (SGLT2i) in kidney transplant recipients: what is the evidence?. Ther Adv Endocrinol Metab 2022; 13:20420188221090001. doi: 10.1177/20420188221090001 [Crossref] [ Google Scholar]
- Bhanushali KB, Asnani HK, Nair A, Ganatra S, Dani SS. Pharmacovigilance study for SGLT 2 inhibitors- safety review of real-world data & randomized clinical trials. Curr Probl Cardiol 2024; 49(9):102664. doi: 10.1016/j.cpcardiol.2024.102664 [Crossref] [ Google Scholar]
- Czerwiński J, Kaliciński P, Danielewicz R. Serious adverse events and reactions in organ transplantation; a web-net tool-based nationwide system for reporting and monitoring. Ann Transplant 2015; 20:243-8. doi: 10.12659/aot.893009 [Crossref] [ Google Scholar]
- Lin Y, Mok M, Harrison J, Battistella M, Farrell A, Leung M. Use of sodium-glucose co-transporter 2 inhibitors in solid organ transplant recipients with pre-existing type 2 or post-transplantation diabetes mellitus: a systematic review. Transplant Rev (Orlando) 2023; 37(1):100729. doi: 10.1016/j.trre.2022.100729 [Crossref] [ Google Scholar]
- McKenzie JE, Brennan SE, Ryan RE, Thomson HJ, Johnston RV, Thomas J. Defining the criteria for including studies and how they will be grouped for the synthesis. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al, eds. Cochrane Handbook for Systematic Reviews of Interventions. Cochrane; 2024.
- Higgins JPT, Morgan RL, Rooney AA, Taylor KW, Thayer KA, Silva RA. A tool to assess risk of bias in non-randomized follow-up studies of exposure effects (ROBINS-E). Environ Int 2024; 186:108602. doi: 10.1016/j.envint.2024.108602 [Crossref] [ Google Scholar]
- Sterne JA, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019; 366:l4898. doi: 10.1136/bmj.l4898 [Crossref] [ Google Scholar]
- McGuinness LA, Higgins JP. Risk-of-bias VISualization (robvis): an R package and Shiny web app for visualizing risk-of-bias assessments. Res Synth Methods 2021; 12(1):55-61. doi: 10.1002/jrsm.1411 [Crossref] [ Google Scholar]
- Dalton JE, Bolen SD, Mascha EJ. Publication bias: the elephant in the review. Anesth Analg 2016; 123(4):812-3. doi: 10.1213/ane.0000000000001596 [Crossref] [ Google Scholar]
- Page MJ, Higgins JP, Sterne JA. Assessing risk of bias due to missing results in a synthesis. In: Cochrane Handbook for Systematic Reviews of Interventions. John Wiley & Sons; 2019. p. 349-74. doi: 10.1002/9781119536604.ch13.
- Deeks JJ, Higgins JP, Altman DG, McKenzie JE, Veroniki AA. Analysing data and undertaking meta-analyses. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al, eds. Cochrane Handbook for Systematic Reviews of Interventions. Cochrane; 2024.
- Halden TA, Kvitne KE, Midtvedt K, Rajakumar L, Robertsen I, Brox J. Efficacy and safety of empagliflozin in renal transplant recipients with posttransplant diabetes mellitus. Diabetes Care 2019; 42(6):1067-74. doi: 10.2337/dc19-0093 [Crossref] [ Google Scholar]
- Schwaiger E, Burghart L, Signorini L, Ristl R, Kopecky C, Tura A. Empagliflozin in posttransplantation diabetes mellitus: a prospective, interventional pilot study on glucose metabolism, fluid volume, and patient safety. Am J Transplant 2019; 19(3):907-19. doi: 10.1111/ajt.15223 [Crossref] [ Google Scholar]
- Gill M, Leung M, Luo CY, Cheung C, Beauchesne A, Chang D. Erythrocytosis and thrombotic events in kidney transplant recipients prescribed a sodium glucose cotransport-2 inhibitor. Clin Transplant 2023; 37(8):e15013. doi: 10.1111/ctr.15013 [Crossref] [ Google Scholar]
- Hisadome Y, Mei T, Noguchi H, Ohkuma T, Sato Y, Kaku K. Safety and efficacy of sodium-glucose cotransporter 2 inhibitors in kidney transplant recipients with pretransplant type 2 diabetes mellitus: a retrospective, single-center, inverse probability of treatment weighting analysis of 85 transplant patients. Transplant Direct 2021; 7(11):e772. doi: 10.1097/txd.0000000000001228 [Crossref] [ Google Scholar]
- Lim JH, Kwon S, Jeon Y, Kim YH, Kwon H, Kim YS. The efficacy and safety of SGLT2 inhibitor in diabetic kidney transplant recipients. Transplantation 2022; 106(9):e404-12. doi: 10.1097/tp.0000000000004228 [Crossref] [ Google Scholar]
- Mahling M, Schork A, Nadalin S, Fritsche A, Heyne N, Guthoff M. Sodium-glucose cotransporter 2 (SGLT2) inhibition in kidney transplant recipients with diabetes mellitus. Kidney Blood Press Res 2019; 44(5):984-92. doi: 10.1159/000501854 [Crossref] [ Google Scholar]
- Maigret L, Basle L, Chatelet V, Ecotiere L, Perrin P, Golbin L. Sodium-glucose cotransporter-2 inhibitor in diabetic and nondiabetic renal transplant recipients. Kidney Int Rep 2025; 10(3):816-27. doi: 10.1016/j.ekir.2024.11.033 [Crossref] [ Google Scholar]
- Quilis A, Gavela E, Kánter J, Castro-Alonso C, Calatayud E, Vivó E. Use of SGLT2i in non-diabetic kidney transplant recipients. Transplant Proc 2025; 57(1):24-6. doi: 10.1016/j.transproceed.2024.12.009 [Crossref] [ Google Scholar]
- Sánchez Fructuoso AI, Bedia Raba A, Banegas Deras E, Vigara Sánchez LA, Valero San Cecilio R, Franco Esteve A. Sodium-glucose cotransporter-2 inhibitor therapy in kidney transplant patients with type 2 or post-transplant diabetes: an observational multicentre study. Clin Kidney J 2023; 16(6):1022-34. doi: 10.1093/ckj/sfad007 [Crossref] [ Google Scholar]
- Sheu JY, Chang LY, Chen JY, Pan HC, Tseng CS, Chueh JS. The outcomes of SGLT-2 inhibitor utilization in diabetic kidney transplant recipients. Nat Commun 2024; 15(1):10043. doi: 10.1038/s41467-024-54171-8 [Crossref] [ Google Scholar]
- Song CC, Brown A, Winstead R, Yakubu I, Demehin M, Kumar D. Early initiation of sodium-glucose linked transporter inhibitors (SGLT-2i) and associated metabolic and electrolyte outcomes in diabetic kidney transplant recipients. Endocrinol Diabetes Metab 2021; 4(2):e00185. doi: 10.1002/edm2.185 [Crossref] [ Google Scholar]
- Diker Cohen T, Polansky A, Bergman I, Ayada G, Babich T, Akirov A. Safety of sodium-glucose cotransporter 2 inhibitors in kidney transplant recipients with diabetes mellitus. Diabetes Metab 2025; 51(3):101627. doi: 10.1016/j.diabet.2025.101627 [Crossref] [ Google Scholar]
- AlKindi F, Al-Omary HL, Hussain Q, Al Hakim M, Chaaban A, Boobes Y. Outcomes of SGLT2 inhibitors use in diabetic renal transplant patients. Transplant Proc 2020; 52(1):175-8. doi: 10.1016/j.transproceed.2019.11.007 [Crossref] [ Google Scholar]
- Attallah N, Yassine L. Use of empagliflozin in recipients of kidney transplant: a report of 8 cases. Transplant Proc 2019; 51(10):3275-80. doi: 10.1016/j.transproceed.2019.05.023 [Crossref] [ Google Scholar]
- Gul W, Naem E, Elawad S, Elhadd T. Successful use of the sodium-glucose co-transporter-2 inhibitor dapagliflozin in patients with renal transplant and diabetes: a case series and literature review. Cardiovasc Endocrinol Metab 2021; 10(4):222-4. doi: 10.1097/xce.0000000000000246 [Crossref] [ Google Scholar]
- Miyazaki R, Miyagi K. Empagliflozin in kidney transplant recipients with chronic kidney disease G3a-4 and metabolic syndrome: five Japanese cases. BMC Nephrol 2022; 23(1):168. doi: 10.1186/s12882-022-02793-9 [Crossref] [ Google Scholar]
- Shah M, Virani Z, Rajput P, Shah B. Efficacy and safety of canagliflozin in kidney transplant patients. Indian J Nephrol 2019; 29(4):278-81. doi: 10.4103/ijn.IJN_2_18 [Crossref] [ Google Scholar]
- Marfella R, D’Onofrio N, Trotta MC, Sardu C, Scisciola L, Amarelli C. Sodium/glucose cotransporter 2 (SGLT2) inhibitors improve cardiac function by reducing JunD expression in human diabetic hearts. Metabolism 2022; 127:154936. doi: 10.1016/j.metabol.2021.154936 [Crossref] [ Google Scholar]
- Cehic MG, Muir CA, Greenfield JR, Hayward C, Jabbour A, Keogh A. Efficacy and safety of empagliflozin in the management of diabetes mellitus in heart transplant recipients. Transplant Direct 2019; 5(5):e450. doi: 10.1097/txd.0000000000000885 [Crossref] [ Google Scholar]
- Muir CA, Greenfield JR, MacDonald PS. Empagliflozin in the management of diabetes mellitus after cardiac transplantation. J Heart Lung Transplant 2017; 36(8):914-6. doi: 10.1016/j.healun.2017.05.005 [Crossref] [ Google Scholar]
- Sweiss H, Selznick L, Contreras J, Long C, Hall R, Bhayana S. Safety and efficacy of sodium-glucose cotransporter-2 inhibitors in solid organ transplant recipients. Prog Transplant 2023; 33(3):261-5. doi: 10.1177/15269248231189880 [Crossref] [ Google Scholar]
- Mahmoud T, Yagan J, Hasan A, Gheith OA, Mostafa M, Rida S. Sodium-glucose co-transporter 2 inhibitors & glucagon-like peptide-1 receptor agonists, efficacy & safety in diabetic kidney transplant recipients. Clin Transplant 2023; 37(12):e15144. doi: 10.1111/ctr.15144 [Crossref] [ Google Scholar]
- Rajasekeran H, Kim SJ, Cardella CJ, Schiff J, Cattral M, Cherney DZI. Use of canagliflozin in kidney transplant recipients for the treatment of type 2 diabetes: a case series. Diabetes Care 2017; 40(7):e75-6. doi: 10.2337/dc17-0237 [Crossref] [ Google Scholar]
- Lemke A, Brokmeier HM, Leung SB, Mara KC, Mour GK, Wadei HM. Sodium-glucose cotransporter 2 inhibitors for treatment of diabetes mellitus after kidney transplantation. Clin Transplant 2022; 36(8):e14718. doi: 10.1111/ctr.14718 [Crossref] [ Google Scholar]
- Mreyoud H, Walter K, Wilpula E, Park JM. The efficacy and safety of sodium-glucose cotransporter-2 inhibitors in solid organ transplant recipients: a scoping review. Pharmacotherapy 2024; 44(6):444-66. doi: 10.1002/phar.2928 [Crossref] [ Google Scholar]
- Hsia DS, Grove O, Cefalu WT. An update on sodium-glucose co-transporter-2 inhibitors for the treatment of diabetes mellitus. Curr Opin Endocrinol Diabetes Obes 2017; 24(1):73-9. doi: 10.1097/med.0000000000000311 [Crossref] [ Google Scholar]
- Madero M, Chertow GM, Mark PB. SGLT2 inhibitor use in chronic kidney disease: supporting cardiovascular, kidney, and metabolic health. Kidney Med 2024; 6(8):100851. doi: 10.1016/j.xkme.2024.100851 [Crossref] [ Google Scholar]
- Talha KM, Anker SD, Butler J. SGLT-2 inhibitors in heart failure: a review of current evidence. Int J Heart Fail 2023; 5(2):82-90. doi: 10.36628/ijhf.2022.0030 [Crossref] [ Google Scholar]
- Lopaschuk GD, Verma S. Mechanisms of cardiovascular benefits of sodium glucose co-transporter 2 (SGLT2) inhibitors: a state-of-the-art review. JACC Basic Transl Sci 2020; 5(6):632-44. doi: 10.1016/j.jacbts.2020.02.004 [Crossref] [ Google Scholar]
- Tsapas A, Avgerinos I, Karagiannis T, Malandris K, Manolopoulos A, Andreadis P. Comparative effectiveness of glucose-lowering drugs for type 2 diabetes: a systematic review and network meta-analysis. Ann Intern Med 2020; 173(4):278-86. doi: 10.7326/m20-0864 [Crossref] [ Google Scholar]
- He G, Yang G, Huang X, Luo D, Tang C, Zhang Z. SGLT2 inhibitors for prevention of primary and secondary cardiovascular outcomes: a meta-analysis of randomized controlled trials. Heart Lung 2023; 59:109-16. doi: 10.1016/j.hrtlng.2023.02.009 [Crossref] [ Google Scholar]
- Katsimardou A, Theofilis P, Vordoni A, Doumas M, Kalaitzidis RG. The effects of SGLT2 inhibitors on blood pressure and other cardiometabolic risk factors. Int J Mol Sci 2024; 25(22):12384. doi: 10.3390/ijms252212384 [Crossref] [ Google Scholar]
- Li M, Yi T, Fan F, Qiu L, Wang Z, Weng H. Effect of sodium-glucose cotransporter-2 inhibitors on blood pressure in patients with heart failure: a systematic review and meta-analysis. Cardiovasc Diabetol 2022; 21(1):139. doi: 10.1186/s12933-022-01574-w [Crossref] [ Google Scholar]
- Usman MS, Siddiqi TJ, Anker SD, Bakris GL, Bhatt DL, Filippatos G. Effect of SGLT2 inhibitors on cardiovascular outcomes across various patient populations. J Am Coll Cardiol 2023; 81(25):2377-87. doi: 10.1016/j.jacc.2023.04.034 [Crossref] [ Google Scholar]
- Limaye AP, Bakthavatsalam R, Kim HW, Randolph SE, Halldorson JB, Healey PJ. Impact of cytomegalovirus in organ transplant recipients in the era of antiviral prophylaxis. Transplantation 2006; 81(12):1645-52. doi: 10.1097/01.tp.0000226071.12562.1a [Crossref] [ Google Scholar]
- Bharuka V, Meshram R, Munjewar PK. Comprehensive review of urinary tract infections in renal transplant recipients: clinical insights and management strategies. Cureus 2024; 16(2):e53882. doi: 10.7759/cureus.53882 [Crossref] [ Google Scholar]
- Kittipibul V, Cox ZL, Chesdachai S, Fiuzat M, Lindenfeld J, Mentz RJ. Genitourinary tract infections in patients taking SGLT2 inhibitors: JACC review topic of the week. J Am Coll Cardiol 2024; 83(16):1568-78. doi: 10.1016/j.jacc.2024.01.040 [Crossref] [ Google Scholar]
- Mejia C, Yadav A. Kidney disease after nonkidney solid organ transplant. Adv Chronic Kidney Dis 2021; 28(6):577-86. doi: 10.1053/j.ackd.2021.10.010 [Crossref] [ Google Scholar]
- Karimzadeh I, Barreto EF, Kellum JA, Awdishu L, Murray PT, Ostermann M. Moving toward a contemporary classification of drug-induced kidney disease. Crit Care 2023; 27(1):435. doi: 10.1186/s13054-023-04720-2 [Crossref] [ Google Scholar]
- Chuang MH, Tang YS, Chen JY, Pan HC, Liao HW, Chu WK. Abrupt decline in estimated glomerular filtration rate after initiating sodium-glucose cotransporter 2 inhibitors predicts clinical outcomes: a systematic review and meta-analysis. Diabetes Metab J 2024; 48(2):242-52. doi: 10.4093/dmj.2023.0201 [Crossref] [ Google Scholar]
- Nishiyama A, Kitada K. Possible renoprotective mechanisms of SGLT2 inhibitors. Front Med (Lausanne) 2023; 10:1115413. doi: 10.3389/fmed.2023.1115413 [Crossref] [ Google Scholar]
- Liptak P, Ivanyi B. Primer: histopathology of calcineurin-inhibitor toxicity in renal allografts. Nat Clin Pract Nephrol 2006; 2(7):398-404. doi: 10.1038/ncpneph0225 [Crossref] [ Google Scholar]
- Garnier AS, Duveau A, Planchais M, Subra JF, Sayegh J, Augusto JF. Serum magnesium after kidney transplantation: a systematic review. Nutrients 2018; 10(6):729. doi: 10.3390/nu10060729 [Crossref] [ Google Scholar]
- Isakov O, Patibandla BK, Christopher KB, Chandraker A, Hod T. Impact of post-transplantation hypomagnesemia on long-term graft and patient survival after transplantation. Kidney Blood Press Res 2022; 47(5):341-53. doi: 10.1159/000522233 [Crossref] [ Google Scholar]
- Peled Y, Ram E, Lavee J, Tenenbaum A, Fisman EZ, Freimark D. Hypomagnesemia is associated with new-onset diabetes mellitus following heart transplantation. Cardiovasc Diabetol 2019; 18(1):132. doi: 10.1186/s12933-019-0939-5 [Crossref] [ Google Scholar]
- Botros SR, Matouk AI, Anter A, Khalifa MM, Heeba GH. Protective effect of empagliflozin on gentamicin-induced acute renal injury via regulation of SIRT1/NF-κB signaling pathway. Environ Toxicol Pharmacol 2022; 94:103907. doi: 10.1016/j.etap.2022.103907 [Crossref] [ Google Scholar]
- Fan G, Lin L, Zuo H, Yan R, Xu C. Sodium-glucose cotransporter 2 inhibitors and contrast-induced nephropathy risk: a meta-analysis. Eur J Clin Pharmacol 2025; 81(3):337-45. doi: 10.1007/s00228-024-03799-y [Crossref] [ Google Scholar]